
The Hospital Rake
Or: How Indian Healthcare Became the World's Most Profitable Misery Machine

The definitive field manual for the ₹17 trillion revolution that will upend how 1.4 billion people live and die.
Part I: The Body in the Morgue
There’s a business model that gets pitched in private equity meetings that sounds, on paper, like the most beautiful thing in the world. The recurring revenue is locked-in, the customers have zero bargaining power, the total addressable market is literally everyone, and the physical infrastructure creates a nearly impenetrable moat. The EBITDA margins are north of 25%. Return on capital employed is magnificent. It is a multi-decade compounding machine.
This business is, of course, a quiet, ongoing horror story. The business is Indian private hospitals.
Let me tell you how it works. Not from the glossy investor presentation, but from the morgue.
The Transaction
Let’s diagram a simple, commonplace transaction in the Indian healthcare market. You have two parties: a Creditor (a mid-sized private hospital in Koramangala, nice website, 4.2 Google rating) and a Debtor (Rajesh Kumar’s family, with a net worth composed primarily of illiquid, generational assets).
The inciting event occurs at 3 AM. A medical emergency, a heart attack, triggers a non-negotiable extension of credit. The Creditor provides six hours of services, including an angioplasty and a stent or two. The specifics are fuzzy. The services, unfortunately, are unsuccessful. At 11 AM, the Debtor’s primary asset-holder, his father, passes away on the operating table.
This is where the transaction gets interesting.
The Creditor presents an invoice for ₹18,40,000 (roughly $22,000). The Debtor’s annual household cash flow is approximately ₹6 lakhs. The invoice, therefore, represents more than 3x their gross annual income. A liquidity crisis is immediate.
The Debtor attempts to restructure the debt.
He proposes a term loan structure (installments). The Creditor, preferring lump-sum payments, says no.
He requests a haircut on the principal, questioning certain, let’s say, discretionary line items like “Miscellaneous surgical supplies: ₹3,42,000.” The Creditor, citing internal policy, says no.
Now we arrive at the crucial leverage point. The Debtor asks to take possession of an asset currently in the Creditor’s custody: his father’s body. The Creditor, in a move of tactical genius, declines to release the asset until the debt is settled in full. The body has been converted into collateral. The hospital has effectively placed a lien on the deceased.¹
For the next seventy-two hours, the morgue functions as a high-stakes escrow account. This forces a series of emergency liquidity events on the Debtor’s side. Ancestral farmland is sold in a fire sale for ₹12 lakhs. An uncle initiates a loan against his Provident Fund for ₹4 lakhs. A brother-in-law liquidates a mutual fund portfolio for the remaining ₹2 lakhs.
On the fourth day, the Debtor settles the account. On the fifth day, the Creditor releases the collateral. The funeral is held.
Let’s analyze this transaction from both sides of the ledger:
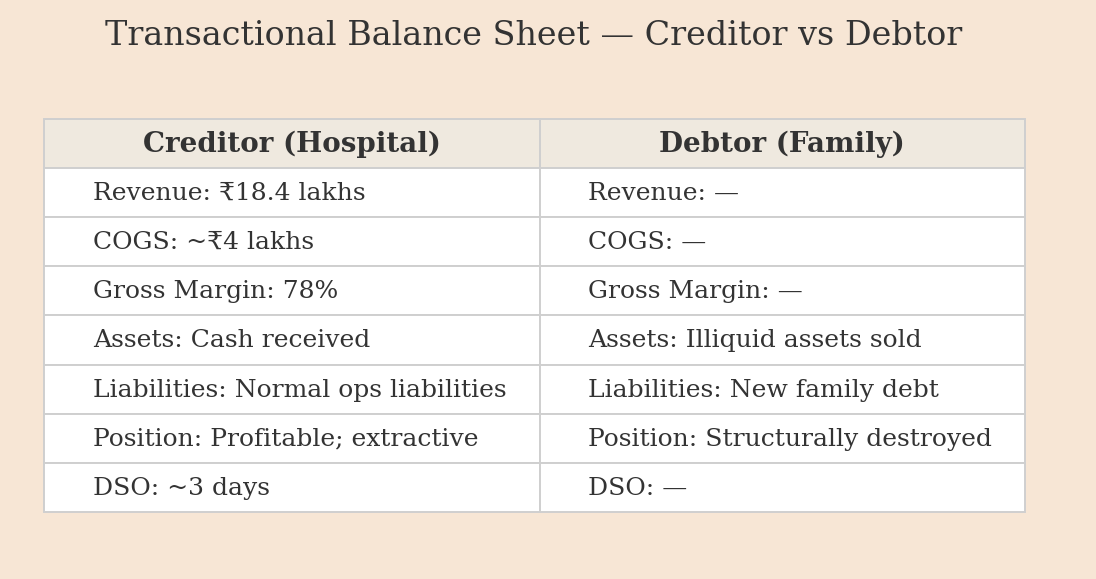
Here is the thing that should make you want to close your laptop and stare into the void: This is not an operational failure or a moral lapse by a rogue employee. This is not a scandal. This is the business model functioning with perfect, ruthless efficiency. The 78% margin is the model. The collateralized body is the collection strategy.
Welcome to Indian healthcare. It’s a beautiful business.
The ₹39 Trillion Arbitrage
Zoom out from that one micro-transaction to the system’s macro balance sheet.
In India, the healthcare industry is funded, to the tune of 47.1%, by emergency capital calls on its customers. This is called Out-of-Pocket Expenditure (OOPE), and it means the system’s revenue is primarily sourced from whatever savings, farmland, or gold a family can liquidate at a moment of extreme duress.
This number is not just high; it’s a structural anomaly. It’s the kind of outlier that suggests you’ve found a mispriced asset. For comparison, the OOPE figures in other, more boring markets are:
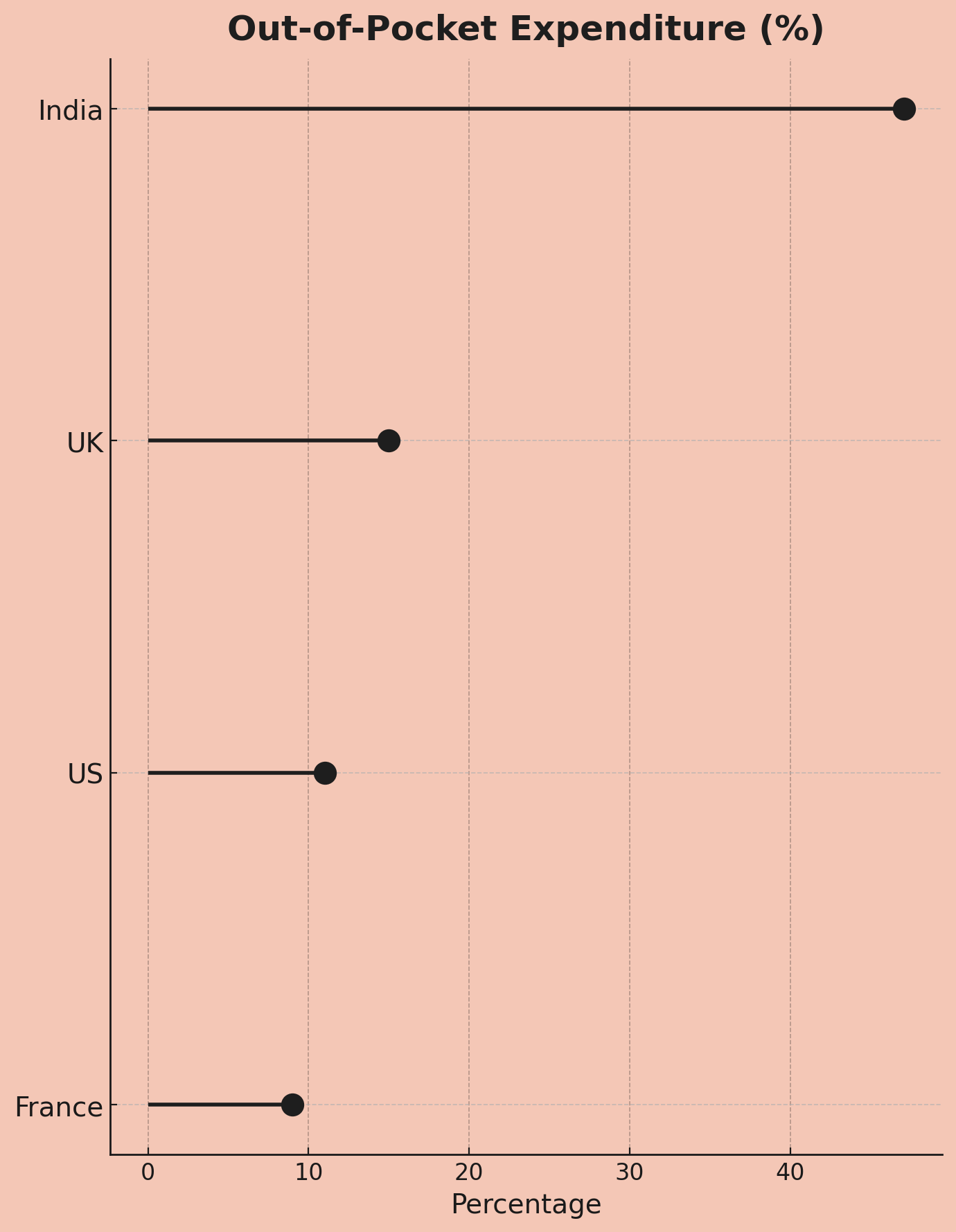
The World Health Organization has a dry, technical term for the output of this model: “catastrophic health expenditure.” In India, this isn’t a rounding error; it’s a predictable, industrial-scale process. Between 32 and 39 million people see their net worth drop below the poverty line each year due to medical bills.
That is the entire population of Canada, liquidated, on an annual basis.
Now, let’s open up the annual reports of the system’s primary beneficiaries: the large hospital chains like Apollo, Fortis, and Max. They are printing 23-25% EBITDA margins. They are private equity darlings. They are, by any rational measure, absolute rocket ships.
So here is the central arbitrage of the Indian healthcare economy: How can a single system be a world-class engine for generating investor alpha and a world-class engine for generating mass poverty, at the exact same time?
The answer, of course, is that it’s not an arbitrage. It’s a direct conversion. One is simply the raw material for the other.
The 25% EBITDA margin is the balance sheet of the 39 million people who were impoverished to create it. The compounding cash flows that investors find so attractive are a clean, dollar-for-dollar ledger of the wealth extracted from millions of households at their most vulnerable. The family’s destroyed future is an externality that doesn’t require disclosure. There is, as of yet, no accounting standard for systemic misery.
To understand the architecture of this perfectly tuned machine, you have to find its source code. You have to find the Original Sin.
Part II: The Original Sin (Or: How Fee-for-Service Became Healthcare’s Flawed Operating System)
The Setup: 1991
Like most well-designed financial disasters, this one began in 1991 with the best of intentions.
India liberalized its economy. The old “License Raj” was dismantled. Capital began to flow. It was, for most sectors, glorious. But in the government’s haste to unshackle the markets, it effectively exited the healthcare business. Public health spending collapsed to a globally insignificant ~1% of GDP. This created a structurally vacant market, a perfect greenfield opportunity. The government’s message was clear: “This is a private sector problem now.”
Capital, which loves nothing more than a vacuum, poured in. A new industry of corporate hospitals was born.
And here, at the moment of creation, the original sin was committed. This new industry needed an operating system, a payment model. It adopted the only one it knew: Fee-for-Service (FFS).
FFS: A Perfectly Perverse Software
Fee-for-Service is a piece of software with one simple, elegant, and deeply perverse directive: maximize Gross Billable Events Per Patient. For every action, a test, a consultation, an incision, the provider logs a transaction and collects a fee.
In theory, this aligns payment with work done. In practice, it creates an incentive structure of almost breathtaking perversity. The system’s KPI is not “patient wellness” or “positive health outcomes.” It is “activity.” The business thrives not on health, but on sickness, and specifically, on the treatment of sickness.
More tests? More revenue.
More procedures? More revenue.
Longer stays? More revenue.
That surgery you might not need? Definitely more revenue.
You might say, “But doctors have ethics!” And they do. But they also have compensation plans. And this is where the software truly shines.
The Principal-Agent Problem, on Steroids
A hospital’s orthopedic surgeons, for instance, are often structured less like doctors and more like commission-based sales agents. They might receive 30-40% of the revenue from every surgery they perform. ²
Let’s model the choice architecture. A patient presents with knee pain.
Option A: Prescribe physical therapy. Revenue: ₹20,000. Surgeon’s Commission: ₹0.
Option B: Recommend a knee replacement. Revenue: ₹5 lakh. Surgeon’s Commission: ₹1.5-2 lakh.
This is not a story about rogue agents but about a perfectly designed principal-agent structure. The hospital (the principal) has designed a contract that incentivizes its agent (the doctor) to maximize the sale of its highest-margin products (surgeries). The agent, acting rationally, complies.
The economists call this “supplier-induced demand.” You might call it a nightmare.
It gets worse. The system has also optimized its pricing engine.
The Estimate Desk
The Estimate Desk: Dynamic Yield Management for Human Suffering
My favorite feature of this model has a certain cartoonish supervillain elegance. Many hospitals operate an “estimate desk,” which is a polite term for a bespoke price discovery unit that operates at the point of maximum emotional leverage. When a patient arrives, typically in an emergency with zero bargaining power, the desk provides an ‘estimate’.
This estimate is not a function of the medical procedure alone. It is dynamically priced based on real-time data signals of the customer’s ability to pay.
Wearing a Rolex? Estimate ↑
Arrived in Mercedes? Estimate ↑
Mentioned insurance? Estimate ↑↑ (hospital knows insurer will negotiate, so start high)
Address in wealthy neighborhood? Estimate ↑
This is textbook price discrimination, the kind of yield management airlines use for seats. Except the variable isn’t your travel flexibility; it’s your desperation to see a loved one survive.
The CAPEX-Incentive Doom Loop
This extractive software runs on hardware whose economics make the whole system inescapable. Building a hospital in a place like Gurgaon is a monster of a financial problem.
Your cost structure:
Land acquisition: ₹800 crores (~$95M)
Construction: ₹500 crores (~$60M)
Equipment: ₹200 crores (~$25M)
Total Day Zero cost: ₹1,500 crores ($180M) before you’ve treated a single patient.
This is largely debt-financed. Your annual debt service, the interest alone, is a cool ₹120–150 crores. That obligation starts on Day 1. Your occupancy rate does not. The relentless pressure of that debt service dictates every operational decision. You must maximize revenue per patient. You must incentivize high-margin procedures. You must set aggressive collection targets.
The hospital isn’t evil. It is simply executing the mandate of its own balance sheet.
This creates a self-reinforcing death spiral: the CAPEX-Incentive Doom Loop.
High Capital Costs create crushing debt.
Crushing Debt demands aggressive revenue targets.
Revenue Targets are met through the FFS incentive software.
FFS Incentives destroy patient finances, but generate the margins and cash flow to...
Attract more capital to build more high-CAPEX hospitals, strengthening the loop.
You cannot fix the incentive problem (the FFS software) without solving the economic problem (the CAPEX hardware). They are one integrated system.
From an investor’s perspective, it’s a business model of exquisite, horrifying beauty. The high out-of-pocket payments mean immediate cash flow with minimal receivables. The massive CAPEX creates an impenetrable moat. The customer has zero pricing power. It’s a machine that turns human desperation into compounding returns.
And for thirty years, it has been humming along perfectly.
Until now.
Part III: The Insurgents (Or: Two Founders Try to Break the Loop from Opposite Directions)
Sometime around 2020, the Indian healthcare doom loop became so obviously, painfully broken that capital began to fund two distinct, almost philosophically opposed, attempts to dismantle it.
Thesis A: The Hardware Fix (SuperHealth). The core problem is economic. The crushing weight of hospital CAPEX is the original sin that forces the entire system into an extractive, FFS model. If you solve the balance sheet, you can afford to run honest software.
Thesis B: The Software Fix (Even Healthcare). The core problem is incentives. The Fee-for-Service operating system is fundamentally corrupt. If you replace the OS with a new one that aligns incentives, the hardware will be forced to adapt or die.
What followed is one of the most fascinating natural experiments in modern business: two brilliant teams attacking the same mountain from opposite faces, only to find themselves converging on the exact same peak.
SuperHealth: The CAPEX Flip
Varun Dubey, SuperHealth’s founder, came from inside the machine (Apollo Hospitals) and then learned about asset-light scaling at a canonical Indian startup (Ola). His insight was simple: what if you applied the Ola model to hospitals? Not by having freelance surgeons, but by unbundling the hospital from its most expensive, illiquid asset: the real estate.
Innovation #1: Lease, Don’t Buy
Instead of building a ₹1,500 crore glass-and-steel temple to medicine, SuperHealth finds the carcasses of the retail apocalypse, defunct Big Bazaars, empty malls, and leases them. They can stand up a fully functional, 50-bed hospital in 125 days.
The financial arbitrage is stunning:
Legacy Model CAPEX/Bed: ₹2 crores
SuperHealth CAPEX/Bed: ₹70 lakhs
This 65% reduction in capital cost is the key that unlocks everything else. It breaks the first link in the doom loop.
Really clever part: By building smaller (50 beds vs 500), SuperHealth can be hyperlocal. Building hospitals like Starbucks, one every few kilometers. Industry builds giant fortresses. SuperHealth builds distributed mesh network.
Trade-off: Can’t do every procedure in 50-bed hospital. No major trauma. No NICU. SuperHealth focuses on secondary care, planned surgeries, diagnostics, short-stay procedures. The stuff that’s 80% of hospital revenue anyway.
But how does 50-bed hospital compete with 500-bed fortress on volume?
Innovation #2: The Throughput Engine
SuperHealth then rejiggers the production line. By focusing on high-volume, short-stay procedures (think cataract, hernia, basic orthopedics), they’ve unbundled the “hospital” from the “hotel.” Their Average Length of Stay (ALOS) is a blistering 1.2 days versus the industry’s 4-5 days.
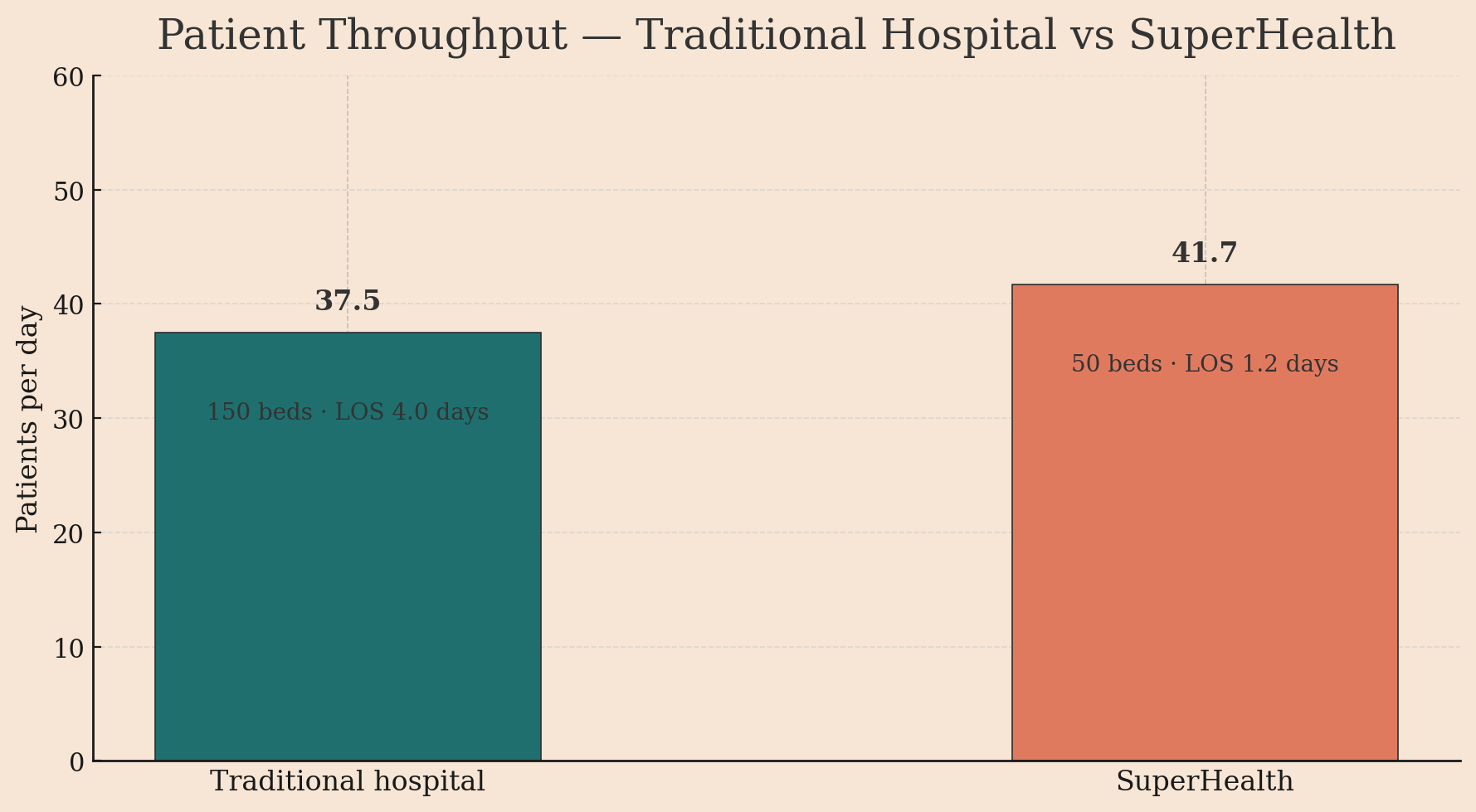
Do the math: a 50-bed SuperHealth facility has a higher patient throughput (41.7 patients/day) than a 150-bed legacy hospital (37.5 patients/day).
They do this by focusing on procedures done under 24 hours:
Cataract surgery (3 hours)
Hernia repair (6 hours)
Diagnostic endoscopy (4 hours)
Most orthopedic procedures (same-day discharge)
Get in, get treated, go home to recover. Works because:
Modern anesthesia improved, you wake up faster
Surgical techniques less invasive means smaller incisions, faster healing
Most complications happen first 6 hours, after that, home is fine
By focusing on high-turnover procedures, SuperHealth processes same volume as traditional hospital with 1/3 the beds. Capital efficiency is insane.
Innovation #3: Zero Doctor Commissions
Because SuperHealth isn’t servicing a mountain of debt, it can afford to do the unthinkable: it pays doctors a salary. Plus equity. This is the magic trick. The doctor’s incentive is no longer to maximize revenue from the patient in front of them, but to maximize the long-term enterprise value of the SuperHealth brand.¹ If the brand wins, their equity prints money. If they destroy trust, they are actively lighting their own money on fire.
The “AWS for Hospitals” Play
The ambition here isn’t to build a few nice, honest hospitals. The ambition is to build 100 of them. This presents a classic scaling problem.
Historically, the quality of healthcare is artisanal. It’s a function of a specific doctor’s hands, a specific team’s chemistry, a specific facility’s culture. You can’t just Ctrl+C, Ctrl+V a great hospital. This is precisely why most large hospital chains struggle with clinical consistency; their 20th hospital is rarely as good as their first.
SuperHealth’s insight is straight out of the manufacturing and cloud computing playbooks: If you can’t scale the artisanal output, you must standardize the inputs.
The tell is their ₹2,500 crore ($300M) deal with United Imaging. This isn’t a simple procurement contract. United Imaging will now supply, install, maintain, and operate the entire radiology stack, MRIs, CTs, X-rays, across all 100 planned SuperHealth hospitals.
Let’s look at the financial engineering here, because it’s beautiful. A single high-end MRI machine is:
Expensive: A ₹15-25 crore line item on the balance sheet.
A Depreciating Asset: Obsolete in 5-7 years.
Operationally Complex: Requires specialized technicians and maintenance contracts.
Chronically Underutilized: Most hospital MRIs sit idle 50-60% of the time.
Traditionally, buying this asset is a terrible use of capital. You tie up millions in a depreciating machine that you don’t even use most of the day.
SuperHealth’s model flips this entirely. It’s a pure CAPEX-to-OPEX conversion. They turn a depreciating asset into a predictable operating expense on their P&L. United Imaging owns the machines, and SuperHealth pays a fee per scan. It’s Equipment-as-a-Service.
But that’s only the first-level genius. The second-level genius is the incentive alignment and network effects.
United Imaging ceases to be just a vendor and becomes a utilization partner. Their profit is now directly tied to maximizing the throughput of the entire SuperHealth radiology network. If one hospital’s MRI is booked solid while another’s idle, United Imaging is incentivized to help dynamically route patients between them. They can run predictive maintenance across the whole fleet, flying one technician to service ten machines in a single trip. They can arbitrage bulk pricing on spare parts.
What SuperHealth has built is a distributed hardware infrastructure with a centralized optimization layer. This is, literally, the Amazon Web Services model applied to medical hardware.
The downstream effects are even more profound. Because every hospital uses the exact same equipment, running the exact same software, the outputs are perfectly standardized. A CT scan from a SuperHealth in Bangalore is the same data object as one from Mumbai. This allows them to build a unified data lake, deploy quality-control AI across the network, and train doctors on a single, universal protocol.
This is how you solve the scaling problem. You don’t build 100 artisanal, one-off construction projects. You build a platform to deploy 100 standardized, repeatable, and infinitely optimizable healthcare factories.
Now for the other insurgent, who started from the opposite end of the stack.
Even Healthcare: The Incentive Flip
If SuperHealth’s thesis is “Fix the economics, and the incentives will follow,” Even Healthcare’s is the inverse: “Fix the incentives, and the economics will be forced to follow.”
Their founders didn’t come from the world of hospital operations; they came from insurance and managed care. They looked at the Indian healthcare machine and saw, not a CAPEX problem, but a fundamentally broken payment protocol. Their conclusion: change the way money moves, and you change everything.
Their model is a simple, radical piece of financial engineering: you pay a subscription.
That’s it. For a single, predictable monthly fee, Even effectively takes on the full liability for a person’s future health. Consultations, diagnostics, surgeries, it all moves from the customer’s P&L to Even’s.
Now, model the incentive structure. It is a perfect, 180-degree inversion of the FFS system.

Even is now, in financial terms, short your future medical bills. They have a direct, powerful incentive to keep that liability as close to zero as possible. Their entire business model moves from episodic treatment to arbitrage through prevention. The ₹500 consultation that catches pre-diabetes is a massive financial win because it prevents a future ₹5 lakh liability.
This, of course, is the classic managed care (HMO) model, the ghost protocol of Indian healthcare. It’s the model that powers giants like Kaiser Permanente in the US. The reason it never took hold in India is that it only works if you can actually control costs.
And this brings us to Even’s strategic quagmire.
The Partnership Trap
Even launched 2020 as digital-first, asset-light. Model:
You pay Even subscription
Even partners with 100+ hospitals across India
When you need care, Even directs you to partner hospital
Even pays hospital (negotiated FFS rates)
Sounds great! Even scales without building hospitals. Hospitals get patient flow. Patients get coordinated care.
Except catastrophic incentive misalignment.
Even’s goal: Keep patient healthy, minimize costs
Partner hospital’s goal: Maximize billable procedures
Every patient interaction becomes negotiation. Even’s care coordinator: “Patient needs follow-up consultation.” Hospital: “Patient needs MRI.” Even: “Protocol doesn’t call for MRI yet.” Hospital: “We’re the doctors, we decide.”
Even trying to run managed care model on top of FFS infrastructure. Like running vegan restaurant in steakhouse. Kitchen optimized for wrong menu.
Gets worse: Hospital knows Even responsible for bill, so even MORE incentive to run up costs. Insurance effect: “Someone else paying, so let’s be thorough” (read: expensive).
Even spent three years trying to make partnerships work. Built sophisticated utilization review. Hired doctors to oversee partner hospital decisions. Negotiated hard on rates.
Wasn’t enough.
Which brings us to July 2025, when Even did something that shocked entire health-tech ecosystem:
They opened their own 70-bed hospital in Bangalore.
Plans for 25 more.
The Full-Stack Pivot
Why would “software” company buy “hardware”? Because they had to.
This was the Full-Stack Pivot. It was a tacit, expensive admission of a fundamental truth: you cannot run superior software on corrupted, legacy hardware. To ensure the integrity of their incentive-aligned OS, they had to build their own vertically integrated machine. The “anti-hospital” company was becoming a hospital company, because it was the only way to build a hospital that could actually run their software.
When you own the hospital:
Doctors salaried, not commission-based
Treatment protocols standardized
Track outcomes longitudinally
Facility optimized for prevention, not procedures
No adversarial negotiation, one system
The irony is delicious: Even Healthcare, which started as “anti-hospital” company, becoming hospital company. Because hospitals aren’t the problem, incentives inside hospitals are the problem.
Even’s hospitals look different, optimized for different business model:
Facility design:
Heavy emphasis on primary care (consultation rooms, not operating theaters)
Diagnostic equipment on-site (blood work, X-rays)
Small inpatient capacity (20-30 beds for short stays)
Connected to telemedicine platform (app doctor = in-person doctor)
Clinical protocols:
Evidence-based guidelines (not “doctor’s discretion”)
Outcomes tracking (every patient’s health trajectory measured)
Preventive care emphasis (health coaching, chronic disease management)
Staffing:
Doctors paid salary, measured on clinical outcomes (patient health improvement, readmission rates)
No commission structure
Long-term employment (building relationships, not transactions)
This is what managed care looks like when you control whole stack.
Fascinating part: Even now building exactly what SuperHealth built from opposite direction.
The Great Convergence
Zoom out. What you are witnessing is a real-time A/B test of two different theories of system change, both arriving at the exact same conclusion.
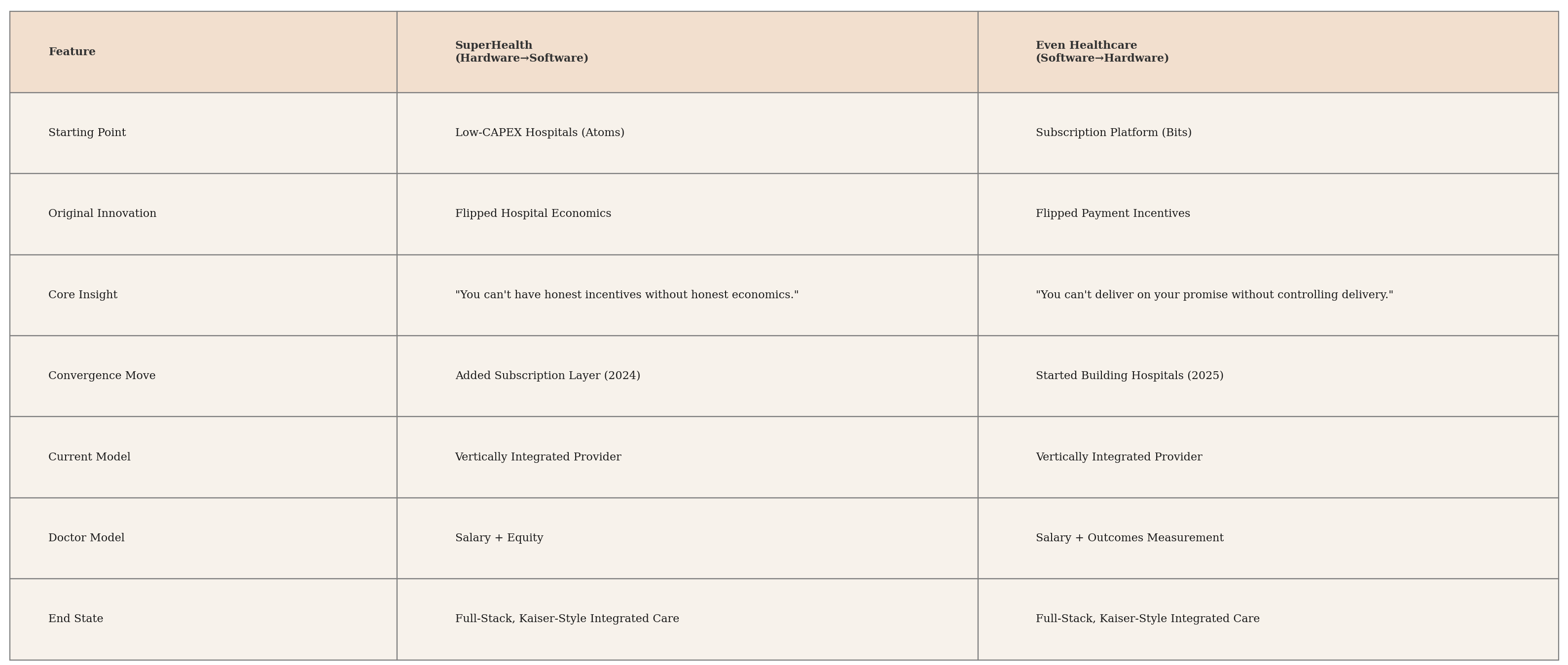
SuperHealth, the hardware-first company, built its low-CAPEX hospitals and then realized that to capture long-term value and build a durable brand, it needed to own the customer relationship directly. In 2024, it bolted on a subscription software layer.
Even Healthcare, the software-first company, built its subscription model and then realized that its product was being corrupted by its reliance on a misaligned hardware layer. In 2025, it began building its own physical infrastructure.
From opposite ends of the universe, they are now building the identical thing: a recurring revenue business sitting on top of a vertically integrated physical infrastructure.
The competing theses: “Fix hardware first” vs. “Fix software first” have converged on a unified theory: in a market this broken, you cannot outsource trust.
Why? Because a partial solution is fatally compromised.
A pure-software play (Even, pre-2025) is a promise you can’t keep. You sell a subscription for “great, affordable care,” but you are contractually dependent on FFS hospitals whose entire business model is to provide “expensive, over-treated care.” The service-level agreement is fundamentally unenforceable.
A pure-hardware play (SuperHealth, pre-2024) is a product nobody trusts. You build a “low-cost hospital,” and the market reasonably assumes it’s low-cost for the wrong reasons (bad doctors, old equipment, cutting corners) because that has been the only model for 30 years.
The only way to solve this trust deficit is to control the entire value chain. To make the promise and own the delivery. From the first premium payment to the last follow-up consultation, it must all run on a single, incentive-aligned stack.
This is, of course, the blueprint for the legendary Kaiser Permanente. Kaiser is both the insurer (the payer) and the hospital system (the provider). This organisation is a piece of beautiful financial engineering. The payer side of the business is naturally short healthcare costs, while the provider side is naturally long them. By integrating them into one entity, you create a perfectly hedged system whose only remaining imperative is to reduce the underlying cost basis, which is just a financial term for “keeping people healthy.”
Finally, the system wants what you, the patient, want.
The Convergence Framework
The competitive question now is: who can traverse the stack faster? Is it easier to add a software layer to a complex physical operation, or to build a complex physical operation to support an existing software business?
My money is on the hardware-first player. Atoms are harder than bits. Building hospitals, even lean ones is a brutal game of real estate, permitting, and supply chains. Even has to learn this from scratch while SuperHealth just needs to hire product managers.
But in the end, who gets there first is less interesting than the fact that they’ve both seen the same map and are heading for the same destination.
The future of Indian healthcare is full-stack, vertically integrated, and incentive-aligned. The revolution requires nothing less.
Part IV: The Enablers
Revolutions are not spontaneous. They are the result of a specific formula: a believable precedent proves a new model is possible, new technology makes it scalable, and new regulation makes it legal.
In the 2020s, Indian healthcare finally has all three
Enabler #1: The Proof of Concept (Dr. Devi Shetty’s “Heart Factory”)
You cannot understand the current insurgency without first understanding its intellectual godfather: Dr. Devi Shetty.
In 2001, Dr. Shetty founded Narayana Hrudayalaya with a mission that sounded, to the prevailing healthcare establishment, completely insane. At a time when cardiac surgery cost ₹2-3 lakhs in India and over $100,000 in the US, he announced his intention to deliver it for ₹60,000 (then about $1,200).
He wasn’t a madman. He was simply the first person to stop thinking like a doctor running a workshop and start thinking like an industrial engineer running a factory. Instead of innovating on the surgery itself, he innovated on the production system for the surgery.
The Narayana System:
Industrialized Scale: A typical hospital might do one or two heart surgeries a day. Narayana does over thirty. This insane volume amortizes the massive fixed costs (operating theaters, equipment) across more units, drastically lowering the cost per unit. It also creates a powerful learning-curve effect: his surgeons became exceptionally good, exceptionally fast.
The Toyota Production System for Thoraxes: The operating theater was redesigned as an assembly line. Surgeons only perform the core surgical tasks. Specialized teams handle preparation, anesthesia, and closing. Operating rooms run back-to-back, minimizing downtime. Every process is standardized and checklist-driven.
Ruthless Capital Allocation: The hospital was built as a clean, functional factory, not a five-star hotel. Zero capital was wasted on marble lobbies or other non-clinical aesthetics. Every rupee was plowed into core production assets: better equipment and more capacity.
Internal Price Discrimination: Wealthier patients were charged more, creating a cross-subsidy that allowed the hospital to offer the same service to poorer patients at or below cost. (Hello, Estimate Desks!)
The results destroyed the central lie of the Indian healthcare system, that cost and quality were an inescapable trade-off.
Cost: Narayana delivered the surgery for ₹60,000-1,00,000.
Quality: Its mortality rates (1.4%) were comparable to the best hospitals in the United States (~1.2%).
Dr. Shetty proved, irrefutably, that you could have both low cost and high quality. They weren’t opposites; they were the twin outcomes of a better-designed system.
So, the obvious question: Why didn’t this model take over the world?
Narayana today is a successful chain of ~30 hospitals, but it is not the dominant force. The constraints were real:
Specialization: The “factory” model is perfectly suited for a high-volume, standardized procedure like cardiac surgery. It’s much harder to apply to the messy, unpredictable world of a multi-specialty hospital.
Culture: The system relies on an intense, almost fanatical operational discipline. Scaling that kind of human culture is notoriously difficult. ³
Capital: Even with a lean model, building 30 hospitals costs billions. Building 1,000 was, at the time, financially prohibitive.
But Narayana’s ultimate contribution wasn’t its own scale. It was that it provided the crucial proof-of-concept. It proved that the doom loop could be broken. It planted the seed of an idea that inspired an entire generation of founders, including Varun Dubey, that a better system was not just imaginable, but achievable.
Enabler #2: ABDM (The Digital Rails)
A modern healthcare system cannot be built on an analog data structure. For decades, Indian healthcare data was trapped in proprietary, disconnected silos: some digital, most in paper-stuffed filing cabinets. A patient’s medical history was effectively the property of the last hospital they visited. This wasn’t a bug but a feature of this system. It created high switching costs and massive information asymmetry, a powerful moat for incumbents.
Then, in 2021, the government began laying down a new set of public rails: the Ayushman Bharat Digital Mission (ABDM).
The vision is to do for healthcare what UPI did for payments: create a single, interoperable protocol for data exchange. Every Indian gets a unique health ID (ABHA number), which functions as a universal primary key. Every medical event: a prescription, a lab result, a discharge summary can be linked to this key, creating a longitudinal, portable health record for every citizen.
For the insurgents, this is less convenience and more a strategic weapon.
It Destroys Data Moats. With ABDM, a patient’s history is no longer held hostage by a hospital. If a customer wants to switch from an Apollo to a SuperHealth, their entire medical file can, in theory, move with them. The old system’s lock-in mechanism is vaporized.
It Creates a Common API for Health. For the first time, it becomes possible to coordinate care across a fragmented ecosystem. A specialist at Hospital A, a lab at Clinic B, and a pharmacy at Location C can all read and write to the same patient file. This interoperability is the prerequisite for building any kind of intelligent, system-wide health platform.
It Enables Competition on Outcomes. This is the killer app. Once patient data is liquid and standardized, it becomes possible to measure and compare things that were previously hidden. Patients could, in the future, see a provider’s verified readmission rates or clinical outcomes. The basis of competition shifts from marble lobbies and marketing budgets to provable quality.
Now, for the reality check. The vision is magnificent; the on-the-ground execution is, predictably, a mess. While over 620 million ABHA IDs have been created, the actual linkage of health records remains in the single digits.
The reasons are a perfect study in incentives:
Incumbent Resistance: Why would a legacy hospital voluntarily adopt a system designed to eliminate its data moat? They have every incentive to slow-roll integration and keep their data proprietary. ⁴
Technical Debt: Many smaller providers simply lack the IT infrastructure to connect to the new rails.
Data Quality: When records are uploaded, they are often incomplete or unstructured. It’s a classic “garbage in, garbage out” problem.
But here’s the crucial point: the system doesn’t have to be perfect to be revolutionary. The mere existence of these rails changes the game.
The insurgents, SuperHealth and Even, are building their entire tech stacks to be ABDM-native from Day One. They want data portability because they are betting they can win on a level playing field. They want outcomes transparency because they believe their outcomes will be better.
The incumbents are playing defense, protecting the moats of the old world. The insurgents are playing offense, building on the rails of the new one.
Enabler #3: Telemedicine Regulations (The Unlock)
For decades, telemedicine in India existed in a state of unpriced legal risk. It wasn’t explicitly illegal, but it wasn’t explicitly legal either. For any serious founder or investor, it was a “pencil’s down” problem. You simply couldn’t build a scalable business on a foundation of regulatory ambiguity.
Then came the black swan.
COVID-19 was a brutal forcing function. In March 2020, with the country in lockdown, the government’s hand was forced. In a scramble, it issued the Telemedicine Practice Guidelines, and overnight, a massive legal grey area was transformed into a clearly defined, permissible activity.
This was the regulatory unlock for the entire software-first healthcare thesis.
For a company like Even Healthcare, the subscription model is only viable if the marginal cost of a “consultation” is driven toward zero. An “unlimited” offering is economically catastrophic if each unit of consumption is a high-cost, in-person event.
Telemedicine fundamentally rewrites the cost curve of primary care.
Legacy Model: A ₹500-1,000 in-person consultation involves real estate overhead, scheduling friction, and limited doctor capacity (maybe 15-20 patients/day).
Telemedicine Model: A video consultation strips out nearly all of that overhead. It’s just the doctor’s time and a sliver of platform cost. The throughput of that same doctor can triple to 50+ consultations/day.
It effectively turns primary care from a high-touch, location-based service into a low-touch, scalable software product.
The Moral Hazard Reversal
This new, ultra-low-cost interaction enables a beautiful piece of economic jujitsu.
In traditional insurance, “moral hazard” is the enemy. When a service is free at the point of use, people tend to over-consume it, driving up costs. The entire industry is built to create friction to prevent this.
The subscription-plus-telemedicine model inverts this. It makes a feature out of the bug. When consultations are “free” and frictionless for the subscriber, they are encouraged to call at the first sign of a problem.
This “over-consumption” of cheap, early-stage care is the system’s most powerful risk-management tool. A ₹100 video call today is an incredible arbitrage against a potential ₹5 lakh hospitalization in the future. The model weaponizes the patient’s tendency to seek care, using it as a data-gathering and early-intervention mechanism.
Yes, there are still limitations: rules around the first consultation being in-person, prescription restrictions, and murky liability frameworks. But the core unlock is done.
The regulatory environment for a foundational piece of the new healthcare stack went from pending_approval to active. The software-first revolution now had a legal API to build on.
Enabler #4: The Unfinished Revolution (Insurance)
Here is the dirty secret: the Indian health insurance industry is a beautifully designed, zero-sum war. And the patient is the battlefield.
On one side, you have the hospitals, running on the Fee-for-Service (FFS) OS. Their mandate is to maximize billable events. On the other side, you have the insurance companies, whose mandate is to minimize payouts. The entire system is an adversarial negotiation over a sick person’s body. The Third-Party Administrators (TPAs) are the hired mercenaries in this war, often incentivized to deny claims. ⁵
This is not a bug. It’s the inevitable outcome of a system where the insurer reimburses the provider on an FFS basis. It is a structure of perfectly misaligned incentives.
The solution is an elegant piece of financial engineering called value-based payment, or capitation. In this model, the provider is paid a fixed fee per person, per year. They are no longer selling procedures; they are selling outcomes. They have effectively taken a long position on their patient’s health. If the patient stays healthy, the provider profits. If the patient gets sick, the provider’s margin erodes.
Finally, everyone: provider, payer, and patient is on the same side of the trade.
So why hasn’t this obviously superior model been implemented? The regulator, IRDAI, has been exploring it for years, but the system is stuck.
Incumbent Resistance: Why would a hospital chain earning 25% EBITDA margins on an FFS model voluntarily switch to a capitation model that might earn 10% by keeping people out of their beds?
Underwriting Risk: You can’t price a capitated plan without good data on future costs. India, until recently, didn’t have that data (see: ABDM).
Adverse Selection: The first people to sign up for an “all you can eat” healthcare plan are the hungriest. This risk can bankrupt a poorly designed plan.
But here’s the strategic masterstroke: Even Healthcare is not waiting for this revolution. It is becoming the revolution.
Even is not trying to sell its software to the legacy insurance companies. It is disintermediating them. By being both the payer (taking the subscription fee) and the provider (managing the care), it has created a closed-loop, fully-capitated system from scratch. It is running a live, direct-to-consumer pilot for the future of the entire industry.
If this pilot works at scale, it creates a powerful forcing function. Legacy insurers will have no choice but to copy the model, or risk becoming obsolete.
This is how true system change happens. It doesn’t come from a top-down regulatory mandate. It comes from a bottom-up insurgent who builds a new, better machine, proves the unit economics, and then drags the entire market into the future.
The timeline becomes clear:
2025-2030: The insurgents prove the D2C capitation model is viable.
2030-2033: The model is de-risked. Progressive insurers and state governments launch their own pilots.
2033-2035: The evidence is overwhelming. Regulation catches up to reality, making value-based payment the default.
2035+: The FFS war becomes a historical relic.
The revolution in insurance won’t be televised, it will be built, one subscriber at a time.
Now we need to talk about why this might all fail.
Part V: The Bear Cases (Or: Every Way This Revolution Could Collapse)
Every magnum opus needs this section. Where we steelman the opposition. Where we’re intellectually honest about what could go wrong.
Because here’s the thing: Most revolutions fail. The insurgents get crushed. The incumbents adapt just enough to survive. The system limps along for another decade.
So let’s talk about every way this could collapse.
Bear Case #1: The Trust Problem (”Cheap = Bad” Is Culturally Embedded)
Thesis: The single greatest moat protecting the incumbent hospital chains is not capital, nor regulatory capture, but a deeply embedded market heuristic: in Indian healthcare, price is the primary signal for quality.
This isn’t irrational consumer behavior; it’s a logical response to decades of operating in an information-asymmetric market. In the absence of reliable, transparent data on clinical outcomes, patients have been forced to rely on proxies. And the most powerful proxy is the price tag. The ₹30 lakh car is probably safer than the ₹10 lakh car. The five-star hotel is probably cleaner than the no-star one.
For thirty years, this has held true in healthcare. The gleaming Apollo with its marble lobby wasn’t just selling luxury by engaging in cost signaling. The conspicuous capital expenditure was a hard-to-fake signal of financial stability and, by extension, a commitment to a certain standard of clinical quality. It was a rational choice for a consumer to believe the expensive hospital was less likely to let them die.
This presents a brutal challenge for the insurgents. Their entire model is based on a positive arbitrage: they claim their lower prices are the result of superior operational efficiency and a leaner capital structure. But the market has been trained to interpret lower prices as a signal of a negative arbitrage: corner-cutting, underpaid doctors, and inferior equipment.
The Playbook to Overcome This:
This is, fundamentally, a go-to-market and brand-building problem. The insurgents aren’t just selling healthcare; they are attempting to re-educate an entire market on how to evaluate quality. Their strategy must be a multi-pronged assault on the old heuristic:
Weaponize Transparency. The only way to beat a bad signal (price) is with a better one (data). The insurgents must relentlessly publish their clinical outcomes: readmission rates, infection rates, patient satisfaction scores. They need to make their data so radically transparent that it becomes the new benchmark for the entire industry.
Manufacture a New Brand Signal. Trust is a function of time and consistency. The brand must be built on years of flawless execution. A single high-profile medical error in the early days could be an extinction-level event, as it would confirm the market’s worst fears about “cheap” healthcare.
Execute a Talent Arbitrage (and Publicize It). The most powerful signal they can generate is convincing a star surgeon from a top-tier hospital to take a pay cut to join their salaried model. This is a public declaration of belief from a credible insider, signaling that the “smart money” in the medical community is betting on the new system.
Find the Wedge Customer. They cannot win the premium customer on Day One. The ₹50 lakh/year family will continue to use price as a safety signal. The strategic wedge is the family earning ₹8-12 lakhs: they are priced out of the premium incumbents but are terrified of the quality in the lower tiers. This is the segment that is most receptive to a new value proposition.
Verdict: This is not a fatal flaw in the business model, but it is the primary go-to-market risk. It requires a brutal, multi-year grind to build a new brand from scratch. The product they are really selling is Trust-as-a-Service, and that is a hard product to scale.
Bear Case #2: The Talent Problem (You Can’t Find 10,000 Ethical Doctors)
Thesis: The insurgents’ elegant financial and operational models are irrelevant if they cannot solve the single biggest input variable: acquiring and retaining high-quality medical talent at scale in a market that has been optimized for a different compensation structure for 30 years.
This is the existential execution risk. A hospital is not its building or its balance sheet; it is the collective expertise of its doctors and nurses. If you cannot solve for the “who,” the “how” and “what” are just theoretical models on a spreadsheet.
Let’s quantify the challenge. SuperHealth’s plan for 100 hospitals requires them to recruit, train, and retain roughly 1,700 physicians and over 8,000 nurses and technicians. The fundamental problem is that the entire existing market for this talent has been conditioned by the Fee-for-Service (FFS) system. They are trying to convert a generation of commission-based free agents into salaried, equity-holding employees.
This presents four structural headwinds:
The Compensation Delta: A top orthopedic surgeon at an incumbent hospital can clear ₹1 crore/year, with a significant portion being variable, performance-based commissions. The insurgent offer is a lower cash salary (e.g., ₹50-60 lakhs) plus a pile of illiquid, high-risk startup equity. For a mid-career doctor with a mortgage, this is a tough trade.
Career Risk: The career path in legacy healthcare is linear and predictable. Joining an unproven startup is a high-variance deviation from that path.
The Adverse Selection Trap: This is the most dangerous risk. Who is most likely to be attracted to a model that doesn’t reward “sales”? It might be the doctors who were never very good at “selling” procedures in the first place. The insurgents could inadvertently be selecting for the bottom quartile of the talent pool, creating a self-fulfilling prophecy of inferior quality.
The Churn Problem: If the model fails to provide sufficient financial or professional satisfaction, it will create a revolving door. High doctor churn is a unit-economic cancer that destroys clinical consistency and brand trust.
The Human Capital Arbitrage Playbook
The insurgents cannot win a head-to-head bidding war for talent. Their entire strategy, therefore, must be to find undervalued or mispriced assets in the human capital market. They are not trying to recruit every doctor; they are trying to build a coalition of specific doctor archetypes who are systematically undervalued by the FFS machine.
Segment #1: The Uncorrupted. Target top residents straight out of medical school. They are clinically skilled but have not yet been financially anchored to the commission model. The pitch: “Practice medicine the way you were taught it was supposed to be.” Lock them in with a four-year equity vesting schedule.
Segment #2: The Burnouts. Target the successful, mid-career FFS doctors who are financially secure but morally exhausted. The product you are selling them isn’t wealth; it’s psychic income, the ability to practice medicine without the guilt of over-treatment, and a more predictable work-life balance.
Segment #3: The Diaspora. Go after the vast pool of Indian doctors trained and working in salaried systems abroad (US, UK, Gulf). Many want to return to India but are repulsed by the local FFS culture. The insurgents offer them a unique proposition: a Western-style professional environment in their home country.
Verdict: This is the single biggest bottleneck to scale. The entire thesis rests on the hypothesis that a sufficient number of high-quality doctors exist in these three segments to staff a national chain. The model’s ultimate success will not be measured in EBITDA margins, but in its doctor retention rate and Net Promoter Score. The early signals that both companies are oversubscribed with applicants are positive, but scaling the human element from dozens to thousands is where most revolutions die. The algorithm is elegant; the wetware is the variable.
Bear Case #3: The Adverse Selection & Risk-Pooling Problem
Thesis: The insurgents’ beautiful unit economics are not the product of genuine operational innovation, but of a clever risk-selection strategy. They are arbitraging the healthiest, lowest-cost segment of the patient population, and their model would collapse if forced to absorb the costs of the system’s statistically inevitable, high-cost tail.
This is the classic, brutal critique of any new entrant in a risk-based business. It’s easy to look like a genius when you only underwrite the good risks.
The accusation manifests differently for each model.
For SuperHealth: The Case Mix Accusation
SuperHealth’s operational model is a high-throughput factory for high-margin, low-volatility procedures: a cataract surgery, a hernia repair. These are the financial equivalent of investment-grade bonds: predictable, short-duration, and low-risk.
The core of the bear case is that their P&L is not built to handle the “junk bonds” of healthcare:
The trauma patient with a multi-week ICU stay.
The oncology patient requiring months of unpredictable treatment.
The diabetic with multiple comorbidities whose simple surgery cascades into a complex, high-cost event.
These are the long-tail, high-cost liabilities that sink hospital balance sheets. If SuperHealth were forced to take on a statistically normal distribution of these cases, would their lean, high-throughput model buckle? Would their 1.2-day Average Length of Stay balloon? Would their margins evaporate?
SuperHealth’s Defense: Their argument is that this isn’t cherry-picking; it’s strategic unbundling. They are not trying to be a full-service, universal hospital. They are a specialized factory. They are unbundling the predictable, high-volume “manufacturing” work of healthcare from the chaotic, bespoke “R&D” and “emergency response” work. This is a legitimate strategic defense, but it also means they are not, in fact, a replacement for the entire system, but rather an optimization layer for its most profitable component.
For Even: The Actuarial Death Spiral
Even’s vulnerability is more acute and existential. Their entire business is a capitated risk pool. They are making an actuarial bet that the premiums collected from their members will exceed the healthcare costs those members generate.
The mortal enemy of any risk pool is adverse selection. The people with the highest propensity to sign up for an “all you can eat” healthcare plan are the ones who intend to eat the most. If Even’s risk pool becomes disproportionately populated with the sickest, most expensive patients, it will enter a classic insurance death spiral: high costs force them to raise premiums, which causes the healthiest members to leave, which further concentrates the risk, which forces premiums even higher, and so on, until bankruptcy.
Even’s Defense Mechanism: They are, by necessity, an insurance company, and they must use the tools of insurance to survive.
Risk-Adjusted Pricing: They cannot offer a single flat price. They must underwrite, charging higher premiums for older members or those with pre-existing conditions.
Careful Underwriting: In the early days, they must be selective about who they allow into the pool, potentially excluding the highest-risk individuals. This, however, puts them in a tricky position: if they are too selective, they are not a healthcare solution but simply an “insurance for the healthy.”
Population-Based Acquisition: The best way to build a stable risk pool is to acquire an entire, statistically normal population at once, for example, by signing up all the employees of a large corporation. This diversifies the risk portfolio instantly.
Verdict: This is a structural and legitimate concern. The only way for the insurgents to counter this critique is with radical transparency. They must publish their data: their case mix index, the average acuity score of their patients, and a demographic comparison of their patient base to the general population. If they want to claim they are solving the healthcare problem, they have to prove they can build a profitable model that serves the sick, not just a walled garden that serves the well.
Bear Case #4: The Diseconomies of Scale
Thesis: The insurgents’ model is a beautiful, fragile jewel that only works at sub-scale. As they grow, the very forces they’ve harnessed will turn against them, and their elegant unit economics will collapse under the weight of organizational complexity and market realities. Success will be its own poison.
This is the “success disaster” scenario. The model works so well at 10 units that they raise a billion dollars to build 100, and in the process of scaling, they inadvertently become a slightly cheaper, less efficient version of the very incumbents they sought to destroy.
The decay will happen across four vectors simultaneously:
The Arbitrage Evaporation (Real Estate & Talent)
The early model is built on clever arbitrage. SuperHealth finds undervalued, distressed real estate. Both insurgents find undervalued human capital (the doctors disgusted with the FFS system). But as you scale from 10 to 100 locations, you are no longer an agile opportunist; you are a predictable, whale-sized player in the market.Real Estate: Landlords are no longer negotiating with a desperate startup; they are negotiating with the future of healthcare. Lease rates will climb. The initial 65% CAPEX advantage will start to erode.
Talent: As you hire hundreds of doctors, you saturate the niche pool of “true believers.” You are now competing for the median doctor, who is more mercenary. This will drive up salaries, shrinking the compensation gap and weakening the model’s cost advantage.
The Decay of Culture and Control (Management)
At 10 hospitals, the founder is a panopticon. They can visit every facility, know every senior doctor, and personally transmit the cultural DNA. At 100 hospitals, this is impossible. You have to insert layers of abstraction: regional VPs, district managers, a professional bureaucracy.The tight, mission-driven culture that produced the initial magic gets diluted.
Principal-agent problems multiply down the chain of command.
The organization begins to develop the very bureaucratic sclerosis it was designed to replace.⁶
The Entropy of Execution (Quality Control)
How do you ensure that Hospital #87 in Ranchi is delivering the same standard of care as the flagship in Bangalore? Without the founder’s direct oversight, and without the sharp, transactional incentive of FFS commissions, what prevents standards from slipping? How do you stop a rogue clinic manager from quietly re-introducing under-the-table incentives to boost their P&L? The system, like all complex systems, will naturally tend toward entropy. Preventing this requires a massive, ongoing investment in quality control systems that adds to the overhead and complexity the model was supposed to avoid. This is the United Airlines Risk: the company grows so fast that its operational quality collapses, and the brand becomes synonymous with the very mediocrity it disrupted.Painting a Target on Your Back (Regulation)
When you are a small, cute innovator, regulators and incumbents ignore you. When you are a rapidly scaling threat to a ₹5 trillion industry, you become Public Enemy Number One. The incumbents will not compete with you on price or quality; that’s too hard. They will compete with you in the halls of government. They will lobby for new regulations designed specifically to kill your model: minimum CAPEX requirements, scope-of-practice restrictions, new licensing hurdles. You go from being an innovator to being a target.
The Mitigation Playbook
This slide into mediocrity is not inevitable, but avoiding it requires a fanatical, almost paranoid discipline.
Scale Oversight with Technology. You cannot scale the founder, but you can scale their oversight. This means building a powerful central nervous system: an AI-driven platform that monitors clinical protocols, flags billing anomalies, and tracks outcomes across the entire network in real time.
Distribute Ownership. You have to fight bureaucracy by aligning incentives at the edge. This means giving local hospital CEOs and lead doctors significant equity, making them partners with skin in the game, not just employees in a hierarchy.
Choose Your Growth Rate Wisely. The ultimate defense is to resist the VC-fueled pressure to blitzscale at all costs. A flawlessly executed network of 30-40 hospitals is infinitely more valuable and defensible than a messy, inconsistent network of 100. This requires a strategic decision to prioritize operational integrity over market share growth.
Verdict: This is the most insidious risk, because it’s a byproduct of success. The core model is sound. The danger is that the physics of corporate gravity will inevitably pull the insurgents back down to the mean. Their greatest challenge is not disrupting the old system, but avoiding becoming it.
Bear Case #5: The Incumbent Counterattack (Apollo Launches “Apollo Honest”)
Bear Case #5: The Innovator’s Dilemma
Thesis: The insurgents are not fighting a startup; they are fighting a dormant giant. The moment their model is de-risked and proven profitable, the giant (Apollo, Fortis, etc.) will wake up, copy the playbook, and use its immense structural advantages: brand, capital, and distribution, to crush them.
This is the classic, terrifying “Innovator’s Dilemma” scenario. The insurgents do all the hard, risky work of market creation, and the incumbent, having watched and learned, swoops in for the kill.
On paper, the incumbent’s advantages are overwhelming:
Brand as a Moat: “Apollo” is a trusted, Schelling point for quality. “SuperHealth” is an unknown quantity.
Cost of Capital: A publicly traded giant can raise billions in debt at low interest rates. The insurgents have to sell expensive equity to VCs.
Distribution & Relationships: The incumbents have decades-long contracts with every major corporation and insurer. They are already embedded in the system.
The War Chest: An incumbent can subsidize a new, low-margin “Apollo Lite” venture for years, bleeding it dry with cash from its profitable core business, an option the insurgents simply don’t have.
So, what stops Apollo from launching “Apollo Honest” tomorrow and ending this revolution before it begins? The answer is that the very structure that makes them powerful also makes them inert.
The Cannibalization Mandate
The FFS model, for all its horrors, prints 25% EBITDA margins. The insurgents’ lean, honest model might print 10-15%. For a public company CEO, launching a new, lower-margin business that will directly compete with and steal customers from your primary cash cow is a structurally irrational act. Your job is to protect margins, not voluntarily compress them. Why would you introduce a product that makes your own business less profitable? ⁷The Incentive & Contractual Hairball
An incumbent like Apollo has thousands of doctors operating under commission-based contracts. This isn’t just a compensation policy; it’s the load-bearing wall of their entire human capital structure. You cannot simply flip a switch and move everyone to a salaried model. Your best, highest-producing “salesmen” would walk. Re-architecting this would require untangling a decade of principal-agent knots, a task so complex and politically fraught that it’s almost unthinkable.The Cultural OS
For forty years, Apollo’s entire corporate organism, from the CFO to the ward nurse has been optimized to answer one question: “How do we maximize Average Revenue Per Occupied Bed (ARPOB)?” SuperHealth’s culture is designed to answer, “How do we maximize patient trust and lifetime value?” These are fundamentally different operating systems. An incumbent cannot simply install a new culture like a software patch; it’s embedded in every process, every KPI, and every middle manager’s quarterly bonus.
To truly compete, the incumbent would have to create a completely separate, walled-off entity: a new brand, new facilities, and a new talent pool. At which point, they are simply building a direct competitor to themselves, begging the question: why not just let the insurgents take the low-margin market while you dominate the premium segment?
Verdict: This is a race against time. The incumbent’s inertia provides a crucial 3-5 year window of uncontested execution for the insurgents. If, within that window, they can build a defensible brand and lock in a critical mass of customers (especially with sticky subscription models), they can survive the inevitable counterattack. If they are still small and fragile when the giant finally wakes up, they will be crushed. The game is to build a moat before the incumbent realizes it’s at war.
Bear Case #6: Regulatory Capture (The Endgame Moat)
Thesis: This is the endgame. When an incumbent cannot win a war on the battlefield of the free market, it moves the conflict to a different venue: the state. This is the weaponization of bureaucracy. The goal is not to build a better product, but to lobby for a set of rules that makes the insurgent’s product illegal.
This is the most potent and cynical of the bear cases, because it has nothing to do with customers or quality. It is pure, brute-force political leverage. The incumbent argument will be cloaked in the language of “patient safety” and “quality standards,” but its true purpose will be to legislate the insurgents out of existence.
The Incumbent’s Political Playbook
The attacks will be surgical strikes on the insurgents’ core operational and economic advantages:
Weaponize ‘Quality’ Standards. Lobby for regulations that define a ‘real hospital’ in terms of the incumbent’s bloated cost structure. Mandate a minimum CAPEX-per-bed that just so happens to be impossible to meet with SuperHealth’s lean, asset-light model. Suddenly, SuperHealth’s innovation is rebranded as “substandard.”
Redefine ‘Scope of Practice’. Introduce rules that tie specific procedures to facility size. For example, “cardiac procedures can only be performed in 500+ bed hospitals.” This kills the insurgents’ smaller, distributed model and forces them to play the incumbent’s high-CAPEX game.
Strangle the Business Model in Red Tape. Argue that Even’s subscription is not ‘healthcare’ but ‘unregulated insurance.’ This triggers a decade-long review by the insurance regulator (IRDAI), effectively killing the model while it’s in the cradle.
Eliminate the Price Advantage. Lobby for price controls or standardized rate cards for all procedures. If SuperHealth is legally required to charge the same as Apollo, its primary competitive vector is gone.
This is not just a theoretical threat. This is the standard defense mechanism for entrenched industries in India, from taxis to telecom.
The Insurgent’s Asymmetric Warfare Doctrine
The insurgents cannot win a traditional lobbying war. They don’t have the war chest or the decades-long relationships. Their only path is to fight an asymmetric campaign.
Achieve Political Escape Velocity. The primary defense is speed. You must scale your customer base, and thus, your voting bloc faster than the incumbents can mobilize their lobbyists. It is much harder for a politician to ban a service that a million of their constituents already love. Your customer base is your political capital.
Build a Human Shield. Form alliances with patient advocacy groups and consumer rights organizations. Frame the public debate as “pro-patient innovators vs. anti-consumer cartels.” Make it politically toxic for any official to be seen siding with the expensive incumbents.
Weaponize the Truth. Use radical transparency on outcomes and pricing as a political tool. Make it blindingly obvious to the public and to regulators that your model delivers better results for less money. It is hard for a government to ban the thing that is provably working.
Exploit the Bugs in the System (Federalism). Healthcare regulation in India is a patchwork of state and central laws. If one state is captured by incumbents, you retreat and scale in a more favorable one. Use the federation’s complexity as a firewall against a monolithic regulatory attack.
Verdict: This is a real and potent risk. The outcome of this battle will be determined by a simple race: can the insurgents acquire a critical mass of patients before the incumbents can acquire a critical mass of politicians? If the insurgents can make their services essential to millions of middle-class voters, they win the lobbying war. If they are still a niche, marginal player when the political attack comes, they will be extinguished.
So, which bear case is most likely to kill the revolution?
My ranking:
Talent Problem (40% probability): Can’t find enough ethical doctors = Can’t scale = Model stays niche
Scaling Problem (25%): Grow too fast, quality collapses, brand destroyed
Trust Problem (15%): Patients never believe “cheap = good,” stick with expensive brands
Incumbent Counterattack (10%): Apollo wakes up, copies model, crushes insurgents with scale
Cherry-Picking Problem (5%): Exposed for only treating healthy patients, credibility destroyed
Regulatory Capture (5%): Government bans model under industry pressure
Combined probability that revolution fails: ~60-70%.
But here’s the thing: Even if SuperHealth and Even specifically fail, the model succeeds. Because they’ve proven it works. Others will copy. The doom loop is broken.
That’s what makes this a real revolution. It’s not about one company winning. It’s about one system replacing another.
Now let’s talk about how to actually build in this space.
Part VI: The Execution Playbook
Okay, enough with the theory. This is the part of the memo where we move from analysis to allocation. You’re a founder or an investor, and you want to build a piece of this future. Where do you start?
Indian healthcare is a full-stack problem, but capital is deployed in tranches and companies are built in stages. You can’t build the entire Kaiser Permanente model on Day One. You need a wedge, an entry point into the value chain that allows you to build a defensible business before you earn the right to integrate vertically.
There are four primary entry vectors.
Vector 1: The Top-of-Funnel Play (Primary Care)
The Thesis: The structural flaw in Indian healthcare is the lack of a trusted, low-cost front door. 80% of health issues can be solved without a hospital, yet patients go straight to the most expensive node in the network. The opportunity is to build that front door and own the customer relationship at the top of the funnel.
The Stack: A hybrid model. A low-friction telemedicine platform for initial contact, paired with a distributed network of small, asset-light physical clinics for when you need to see a doctor in person.
The Economics: The prize isn’t the transactional margin on a single ₹500 consultation. That’s a low-margin, high-volume game. The prize is the pivot to a subscription model. Once you are the trusted primary care provider for 10,000 families, you can offer an “all-you-can-eat” primary care plan for a recurring fee, creating a predictable, high-LTV revenue stream.
The Moat: A trusted brand and a sticky, recurring relationship with the customer.
The Risk: This is a brutal, high-churn customer acquisition game. You are fighting against a deeply ingrained cultural habit of going straight to specialists.
Founder Archetype: The consumer tech operator. This is a CAC/LTV optimization game more than a medical problem. Think ex-Swiggy/Flipkart growth leads.
Vector 2: The “Intel Inside” Play (Diagnostics)
The Thesis: The diagnostic layer of the healthcare stack is a classic case of underutilized capital assets. Every hospital has its own lab, running at 30% capacity. This is an arbitrage waiting to happen. Standalone, centralized “factories” can process tests at a fraction of the cost.
The Stack: A hub-and-spoke logistics network. A large, centralized lab for processing, surrounded by a constellation of hyper-local collection centers and mobile phlebotomists.
The Economics: These are software-like gross margins. A blood test panel that costs ₹300 to process can be sold for ₹1,500. The entire business is a game of driving volume to maximize the utilization of the central factory.
The Moat: Economies of scale and logistical efficiency. Once you are the lowest-cost provider, you can become the B2B backend for everyone else: hospitals, insurers, and primary care clinics.
The Risk: This is a highly commoditized, price-sensitive market. You are competing with giants like Dr. Lal PathLabs and Thyrocare, who are engaged in a race to the bottom on price.
Founder Archetype: The supply chain and operations wizard. This is a problem for the ex-Delhivery/Amazon logistics manager who gets excited about route optimization and asset utilization.
Vector 3: The Full-Stack Wedge (Specialty Hospitals)
The Thesis: Instead of starting at the low-margin top of the funnel, you start with the hardest, most capital-intensive part: the hospital itself. But you re-engineer it from the ground up to be a lean, high-throughput machine. This is the SuperHealth playbook.
The Stack: Arbitrage distressed commercial real estate. Build smaller, 50-100 bed facilities. Convert every possible piece of CAPEX to OPEX (e.g., Equipment-as-a-Service). Focus on a narrow band of high-volume, predictable procedures.
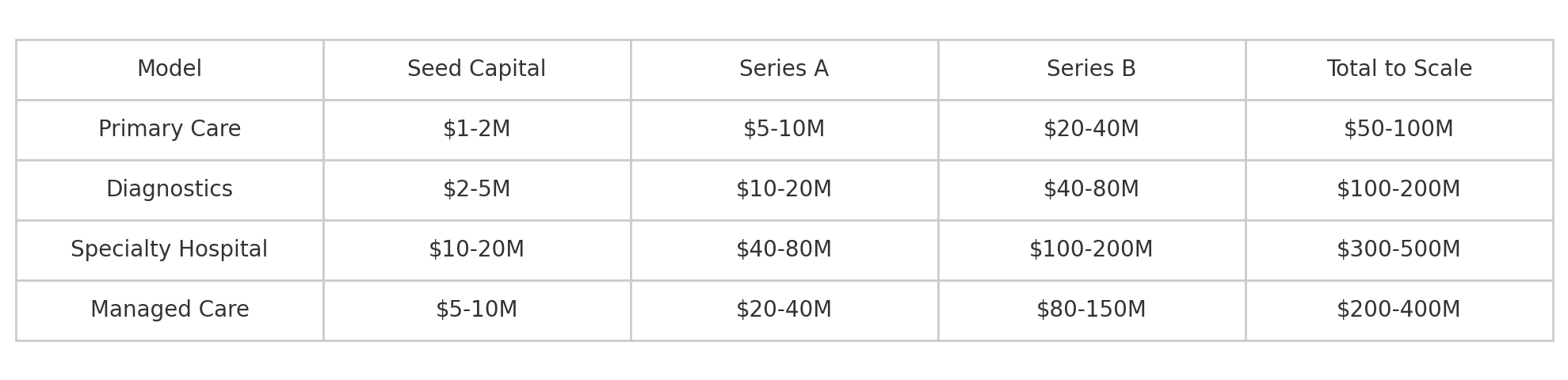
The Economics: This isn’t a venture-scale business in its early days; it’s more of a private equity play. It requires significant upfront capital (₹35-70 crores per facility), but if executed correctly, it can achieve a 3–5-year payback period and generate stable, 15-20% EBITDA margins.
The Moat: Real, physical assets and deep operational excellence. This is the hardest model to copy.
The Risk: This is an execution-heavy, atoms-based business. It’s slow, capital-intensive, and carries significant talent risk.
Founder Archetype: The gray-haired operator. This is a game for the ex-hospital CEO or the real estate developer who knows how to get things built in the real world and can raise serious capital.
Vector 4: The God Mode Play (Managed Care)
The Thesis: This is the most ambitious and dangerous play. You ignore the existing value chain and go straight for the endgame: fixing the incentive problem at its source by becoming both the payer and the provider. This is the Even Healthcare playbook.
The Stack: You start as a “Virtual Integrated Provider,” using a subscription model and a software layer to manage care through partners. Then, as your subscriber base grows, you slowly, painfully, acquire the atoms, building your own clinics and hospitals to control the full stack.
The Economics: This is a pure underwriting game. Your profit is the spread between the premiums you collect and the cost of the care you deliver. The entire business is a bet that you can manage your Medical Loss Ratio (MLR) better than anyone else.
The Moat: A perfectly aligned system with powerful network effects and high switching costs. Once you reach scale, this is the most defensible model in all of healthcare.
The Risk: Existential. You are, in effect, an unregulated insurance company. A single, poorly managed risk pool can lead to an actuarial death spiral and bankruptcy. This requires the most capital and carries the highest risk of catastrophic failure.
Founder Archetype: The finance/insurance nerd with a stomach for existential risk. This is a game for the ex-actuary or hedge fund analyst who sees healthcare not as a service, but as a portfolio of risks to be managed.
Capital requirements by model:
The Talent Playbook
This is the primary constraint. Your elegant business model is a spreadsheet fantasy until you solve the human capital problem. Let me be explicit about how to think about this.
You are not just “hiring doctors.” You are executing a human capital arbitrage strategy. You cannot win a head-to-head cash compensation war against the FFS machine. Your entire playbook must be based on identifying and acquiring high-quality talent that is systematically mispriced or undervalued by the incumbent market.
Part 1: Acquiring the Clinical Assets (Doctors)
You are building a portfolio of clinical talent from three distinct, inefficiently priced market segments.
Segment 1: The Un-Corrupted Asset (New Graduates)
The Asset: Final-year residents from top medical colleges. They are clinically proficient but have not yet had their compensation expectations anchored to the FFS commission structure.
The Arbitrage: You are acquiring high-potential talent before the market has a chance to corrupt it. You are trading on their preference for mission and professional integrity over immediate cash maximization.
The Playbook: Target them aggressively on campus. Offer a clear alternative to the “sales” culture they are about to enter.
Segment 2: The Geographic Arbitrage (Tier 2/3 Returnees)
The Asset: Doctors trained in top-tier metro hospitals who have a non-financial preference to live in their hometowns.
The Arbitrage: You are acquiring a premium, metro-trained asset at a discounted, Tier 2 market price. Their “quality of life” preference is a market inefficiency you can exploit.
The Playbook: Build your early, non-metro hospitals specifically in cities known for exporting medical talent. You become the default “best option” for a high-quality doctor wanting to move home.
Segment 3: The System-Mismatch Asset (The Diaspora)
The Asset: Indian doctors working in salaried, evidence-based systems abroad (US, UK, Gulf) who want to return.
The Arbitrage: These are premium assets that are functionally incompatible with the Indian FFS market. You are the only bidder for this high-quality, ethically-trained talent pool.
The Playbook: Offer a “soft landing” package: a professional culture they recognize, assistance with navigating the Medical Council’s bureaucracy, and a solution to the “moral compromise” problem that keeps them abroad.
The Compensation Stack & The Pitch
Your offer is not just a salary; it’s a different kind of deal.
The Stack: A cash salary that is competitive but likely 10-20% below the all-in FFS equivalent, plus a meaningful grant of equity (0.1-0.5% for early, key hires) with a standard 4-year vest. The equity is the key to creating long-term incentive alignment, turning the agent into a principal.
The Pitch: You are offering an exit from a broken system and a chance to build the new one. The most powerful part of the pitch is not the mission, but the math: “Let us show you our unit economics. This is the financial model for why we don’t need you to be a salesman. We profit from efficiency and trust, not volume.”
Part 2: Acquiring the Operating System (Management)
You need a management team that is a hybrid of three distinct corporate DNAs.
The Frameworks (ex-McKinsey/Bain/BCG): You need the strategy consultants for their analytical rigor and their repeatable playbooks for scaling. They are the architects.
The Scaling Engine (ex-Ola/Swiggy/Flipkart): You need the startup veterans for their logistics-at-speed muscle memory and their experience in the brutal, chaotic reality of 0-to-1 execution in India. They are the builders.
The Domain Expertise (ex-Apollo/Fortis/Narayana): You need the industry insiders to de-risk the clinical operations and provide credibility. They are the domain experts who know where the bodies are buried.
The Ideal Founding Stack
The perfect founding team is a balanced portfolio of these archetypes:
CEO: A seasoned operator who has built something from nothing before and can integrate these disparate cultures.
Chief Medical Officer: A respected senior physician who can serve as the ultimate recruiting tool for other doctors.
CTO: A product and tech leader who understands how to build the technology that will allow the system to scale without collapsing.
CFO: A finance expert obsessed with the numbers, who ensures the revolutionary model remains profitable and doesn’t drift back toward the old ways.
The Regulatory Playbook
This is the non-clinical risk that keeps founders up at night. Regulation is not a checklist; it’s a game board. Here’s how to play it.
Playbook 1: The Bureaucratic Stack for Atoms (Opening a Hospital)
Before you treat a single patient, you must satisfy a multi-layered stack of bureaucratic approvals. This is a non-negotiable, friction-heavy process. The checklist of tollbooths includes:
The Clinical Establishments Act
The Municipal Corporation License
The Fire Department NOC
The Biomedical Waste Management Approval
The Pollution Control Board Clearance
...and several others.
The timeline for navigating this stack is a variable function of your local “consulting” budget.
Normal: 9-12 months.
Slow/Unlucky: 18-24 months.
Accelerated: 4-6 months.
This brings us to a non-negotiable line item in your Series A budget: the local “consultant.” This is typically a former government official who understands the system’s undocumented APIs. For a fee of ₹5-10 lakhs, they provide “friction reduction as a service.” This is not a bribe; it is the market rate for accelerating administrative processes.⁸
Playbook 2: The Great Regulatory Arbitrage (The Subscription Model)
This is where the real high-stakes game is played. The managed care model exists in a beautiful, terrifying regulatory grey area.
The Arbitrage: You are selling a product that, to the customer, feels like insurance, but to the regulator, is legally structured as a “pre-paid healthcare service membership.” This is a crucial distinction. It keeps you out of the clutches of the insurance regulator, IRDAI, whose approval process can take 3-5 years and requires a ₹100 crore capital reserve.
The Risk: The sword of Damocles is reclassification. If you get big enough, IRDAI could wake up and decide that your “membership” is, in fact, a “risk-pooling product,” and retroactively subject you to their entire regulatory regime. This is an existential threat.
The Strategy: Lexical Arbitrage & Escape Velocity
Your defense is twofold. First, you engage in careful lexical arbitrage.
It’s not “insurance,” it’s a “healthcare membership.”
It’s not a “premium,” it’s a “subscription fee.”
It’s not “coverage,” it’s “included services.”
Second, your goal is to grow so fast that you achieve political escape velocity. The strategy is to stay under the radar until you are so big, and have so many happy customers (voters), that reclassifying you and potentially shutting you down becomes politically unpalatable.
Playbook 3: Federalism as a Feature (The State-Level Sandbox)
Healthcare is a “concurrent list” item in the Constitution, meaning both central and state governments have a say. This bureaucratic mess is actually a strategic advantage.
The Sandbox: India is not one regulatory market; it’s 28. This allows you to A/B test your model.
Friendly States (Your “Go-Live” Markets): Start in places like Karnataka or Telangana, where the bureaucracy is relatively efficient and the government is actively pro-innovation. Prove the model here. De-risk the business.
Difficult States (Your “Expansion” Markets): Avoid places like Delhi (political spaghetti), West Bengal (bureaucratic quicksand), or UP (requires deep local alliances) until you have the scale, capital, and a proven playbook to navigate them.
The strategy is simple: find the path of least resistance, build a fortress there, and then use that established base to expand into more hostile territory.
Part VII: The 10-Year Roadmap (Or: How India Gets to Universal, Affordable, Quality Healthcare)
This is the “how it plays out” slide. We’re moving from static analysis to a dynamic model of the future.
Phase 1: The De-Risking (2024-2026)
This is the proof-of-concept phase, where the insurgents prove their spreadsheets can survive contact with reality.
What Happens: The first handful of insurgent hospitals and managed care pods go live. SuperHealth is running 10-15 facilities; Even has 30,000 subscribers and its first few owned clinics. Crucially, they begin publishing their first datasets on clinical and financial outcomes.
The KPIs to Watch (This is the de-risking):
SuperHealth: Can they prove >15% EBITDA margins on a low-CAPEX base? Is their Revenue Per Bed sustainable?
Even: Can they keep their Medical Loss Ratio (MLR) below 80% without aggressive cherry-picking? Can they retain >70% of their subscribers annually?
What This Proves: It proves that the central thesis is not a fantasy. That the unit economics of an “honest” model actually work.
The Market Reaction:
Incumbents: They will publicly dismiss it as a “niche play,” because the alternative, that their entire business model is a dinosaur, is too terrifying to contemplate.
Capital: The scent of blood is in the water. The first “copycat” startups get funded. The successful insurgents raise massive Series B/C rounds.
Phase 2: The Blitzscale (2027-2029)
The model is de-risked. Now comes the land grab.
What Happens: The insurgents pour capital into aggressive expansion. SuperHealth is a 50+ hospital chain. Even is a 200,000+ member organization. This is the period of maximum operational stress.
The Systemic Shift:
Data Liquidity: ABDM finally reaches critical mass. Patient data starts to flow, enabling real, outcomes-based competition for the first time.
The First Cracks in the Old System: Seeing the insurgents’ success, the first progressive insurance companies launch their own capitation pilots. The regulator, IRDAI, is “forced” by the success of these new models to issue official guidelines.
The Convergence Accelerates: The insurgents’ business models become nearly indistinguishable. SuperHealth has a mature subscription product. Even has a significant physical footprint. They are now true, full-stack competitors.
The Incumbent Response: The denial phase is over. The panic begins. They are forced to respond with hastily assembled “value brands” (e.g., “Apollo Care”) and defensive partnerships. The presence of a low-cost, high-quality alternative starts to put real downward pressure on pricing in major metros.
Phase 3: The Flippening & Incumbent Triage (2030-2033)
This is the moment the new system becomes the default.
What Happens: The full-stack, integrated care model is no longer the “insurgent” model; it’s just the modern model. A handful of national players now control 30-40% of the private market. The FFS system is relegated to a niche for ultra-complex procedures. The national Out-of-Pocket Expenditure (OOPE) rate finally bends, dropping from 47% into the 30s, still high, but a generational improvement.
The Kaiser Moment: By 2032, India has its own version of Kaiser Permanente. A system where the payer and provider are one, where incentives are aligned to health, and where the costs are 40-60% lower than the old model. This is what winning looks like.
The Incumbent Triage: The legacy hospital chains face a brutal choice:
Radical Surgery: Attempt a painful, multi-year, bet-the-company restructuring to become a full-stack provider themselves.
Palliative Care: Cede the mass market, retreat to the premium/luxury segment, and manage the graceful decline of their FFS cash cow.
Death.
Phase 4: The Export (2034+)
This is the bull case that gets you a trillion-dollar valuation.
The Thesis: If you can build a low-cost, high-quality healthcare model that works in a market as structurally hostile and economically constrained as India, you have forged a weapon that can win anywhere. The Indian playbook becomes a product to be exported.
The Target Markets: You go after every market with similar structural problems: Southeast Asia (Indonesia, Philippines), South Asia (Bangladesh, Pakistan), Africa (Nigeria, Kenya), and Latin America (Brazil, Mexico). This is a 2.5 billion person addressable market.
The Product: You are exporting a stack:
The Low-CAPEX Hospital Construction Playbook.
The Equipment-as-a-Service Financial Model.
The Managed Care Software Platform & Protocols.
The Endgame: Could an Indian company become the world’s largest healthcare provider? Let’s do the back-of-the-envelope math. 30% of the Indian market plus just 10% of the other similar emerging markets gets you to over 500 million patients under care. The revenue would be north of ₹1 trillion. This would create a company larger than UnitedHealth Group, the current global leader.
This is the prize. Not just to fix a broken system in one country, but to build a new, globally dominant model for the 21st century.
Part VIII: The International Comparisons (What India Can Learn, What India Can Teach)
No revolution happens in a vacuum. To understand the scale and shape of the Indian opportunity, you have to benchmark it against the three dominant global models for private healthcare: the Hospitality & Arbitrage Play, the Integrated System Play, and the State-Capitalism Play.
1. The Hospitality & Arbitrage Play (Thailand, Singapore, Turkey)
This is the business of arbitraging global price and quality differentials. The model is to sell Western-quality healthcare at emerging-market prices, wrapped in a five-star hospitality experience.
The Thai Model: The undisputed volume leader. Their stack is a combination of JCI-accredited quality, a deep ecosystem of facilitators, and a government that actively promotes the industry. They are the Toyota of medical tourism: reliable, affordable, and scaled.
The Singaporean Model: The premium, high-margin player. Singapore is the “Asian Switzerland” of healthcare, selling trust, stability, and access to some of the world’s best clinical institutions. Their secret weapon is Temasek, the state sovereign wealth fund, which owns major hospital chains, creating a powerful, system-wide alignment.
The Turkish Model: The near-shore, specialized arbitrageur. They leverage their geographic proximity to Europe to dominate high-margin, consumer-driven procedures like hair transplants and cosmetic surgery.
The Playbook to Import:
India has the raw materials to compete but has been terrible at packaging and marketing. The insurgents can steal this playbook:
Buy the Badge (JCI Accreditation): The Joint Commission International accreditation is a marketing and compliance cost required to access the global insurance market. An insurgent like SuperHealth should get its first hospital accredited and make it a centerpiece of its brand, signaling that its low costs are not a result of low standards.
Bundle the Product: The product is not just a “surgery” fashion it as a “medical travel package.” Partner with airlines and hotels. Create product bundles like “Cardiac Surgery + One Week Recovery in Goa.” Make the entire experience seamless and managed. There are startups like The Medical Travel Company attempting just that.
India’s Asymmetric Advantage:
The reason India could ultimately dominate this market is scale. The medical tourism business in Thailand is built on a domestic population of 70 million. India has a 1.4 billion person domestic market to serve as the base load for its healthcare factories. This allows for economies of scale that no other country can match, creating a structural cost advantage even over Thailand.
2. The Integrated System Play (Kaiser Permanente, a.k.a. The God Mode)
This is the theoretical holy grail of healthcare, and it actually exists in the wild. Kaiser Permanente is a piece of beautiful financial engineering.
It owns the insurance plan (the payer).
It owns the hospitals and clinics (the provider).
It’s a perfectly hedged system. The payer side of the business is structurally short healthcare costs (it profits when costs are low), while the provider side is structurally long them. By combining them into a single entity, Kaiser created a closed loop where the only rational path to increasing profit is to reduce the underlying liability, which is just a financial term for keeping people healthy.
The results are staggering, costs are 20-30% lower than the US average, and clinical outcomes are consistently superior.
The question is, why isn’t this the global standard? In the US, it’s a combination of regulatory fragmentation and the fact that it’s nearly impossible to retrofit an integrated model onto an existing, adversarial FFS system.
But India doesn’t have this legacy baggage. It is a greenfield opportunity. The insurgents are not trying to fix a broken Kaiser; they are building the Indian Kaiser from scratch.
Why the Indian Version Could Be Bigger and Faster:
For-Profit vs. Non-Profit: Kaiser is a non-profit, which limits its access to growth capital. ⁹ The Indian insurgents are for-profit, venture-backed machines built for speed and scale.
Digital-Native vs. Legacy: Kaiser took 70 years to reach 12 million members. An Indian insurgent, built on a modern, digital stack, could plausibly reach that scale in 15-20 years.
3. The State-Capitalism Play (China’s Parallel Universe)
China is running a parallel experiment with a similar set of problems (a fragmented, FFS-driven system with low trust) but a wildly different OS.
Their insurgency is being driven by their national tech champions: WeDoctor, Ping An Good Doctor, and Ali Health, who are pouring billions into building full-stack, tech-first healthcare ecosystems.
What India Can Learn:
The Power of Platforms: The Chinese players are building multi-sided platforms that integrate patients, doctors, hospitals, and insurers from Day One.
The National Champions: The entry of giants like Alibaba and Tencent signals the strategic importance of the sector. The Indian equivalent would be a full-throated entry by Reliance or Tata.
India’s Asymmetric Advantages:
Permissionless Innovation: China’s state-led model can be powerful, but it also creates bottlenecks. India’s chaotic, fragmented market is a bug that is also a feature: it allows for more rapid, bottom-up experimentation.
Access to Global Capital: Indian startups can raise capital from anyone. Chinese companies face a more complex geopolitical and regulatory landscape.
The Urgency Delta: China, for all its problems, has a more robust public health infrastructure. India’s system is more acutely broken. And acute necessity is the mother of all innovation.
The verdict? Both countries are racing toward the same full-stack, tech-enabled solution. The winner will likely become the default healthcare model for the emerging world. My bet is on India. The combination of a more acute problem, a more entrepreneurial culture, and a more open capital market gives it a slight edge in this generational race.
Part IX: The Final Verdict (The Go/No-Go)
Let’s be direct. This entire document is an investment thesis. And now we come to the final, crucial question: should you, the founder or the allocator of capital, actually make the trade?
Here is the framework for that decision.
The “Go” Signal: The Founder-Market Fit Requirements
You should only attempt to build in this space if you meet a specific, non-negotiable set of criteria. This is not a market for tourists.
1. Your Time Horizon is Measured in Decades.
This is not a SaaS play you can flip in 3-5 years. This is a generational hold. The regulatory moats, the trust deficit, and the sheer physics of building in the real world mean this is a slow, compounding game. If you aren’t prepared to dedicate the next 10-15 years of your life to this, do not start.
2. Your Definition of a Seed Round is ₹100 Crores.
The asset-light, pure-software plays at the top of the funnel are already a red ocean. The defensible, full-stack models that actually solve the problem are games of atoms, not just bits. They are capital-intensive. If you cannot map a credible path to raising ₹100 crores+, you are bringing a knife to a gunfight.
3. You Are a Magnet for a Specific, Contrarian Talent Pool.
The core constraint on this entire model is human capital. Your primary job as a founder is not to build hospitals; it’s to convince a critical mass of the most ethical, talented doctors in the country to take a massive career risk and a short-term pay cut. If you cannot recruit the first ten “true believers,” you will never scale to a thousand.
4. You Have a Maniacal Obsession with Operational Physics.
Healthcare is a business of supply chains, staffing ratios, and biomedical waste management. It is a world of brutal, real-world execution. A beautiful app is irrelevant if your sterilization protocols fail. If you don’t have a founder who gets genuinely excited about optimizing janitorial contracts, find one.
5. You Have the Moral Balance Sheet to Underwrite Death.
This is the tail risk that is not on any cap table. When a SaaS app has a bug, you have a support ticket. When your system fails, people die. The bug reports are obituaries. If you are not emotionally and ethically prepared to carry that weight, do not enter this business.
The “No-Go” Signal: The Disqualifiers
Conversely, you should immediately walk away if any of the following apply.
You Are Looking for an Easy Win. This is Hard Mode. The regulatory environment is a swamp, the incumbents are hostile, and the customer is traumatized.
You Are Chasing a Quick Exit. The investors who understand this space are signing up for a 10-15 year hold. They are not looking for a 5x return in 3 years; they are underwriting a 100x return in 15.
You Are a Purely Rational Financial Actor. This is the paradox. While the opportunity is enormous, the daily temptation to compromise, to introduce a small, hidden commission here, to cut a corner there, will be immense. A purely rational actor would, over time, inevitably drift back toward the old FFS model because it is so damn profitable. ¹⁰ to resist this, you need a non-financial, almost irrational belief in the mission.
The Prize
If, after all that, you are still at the table, then here is the prize.
You are attacking a ₹17.5 trillion market that is structurally broken and begging for a solution.
You have a 10-15 year window of competitive grace before the incumbents can fully adapt.
You have the opportunity to build a trillion-dollar company that is not morally ambiguous, a company that generates alpha by reducing human suffering.
This is not a business for everyone.
It is for the builders who understand that incentives are more powerful than intentions. That low cost and high quality are not a trade-off, but the output of a superior system. That it is possible to get outrageously rich by fixing a problem that actually matters.
If that’s you, then build it.
Conclusion: The Rake, Inverted
Let’s come full circle.
Let’s rerun the transaction from the beginning, but this time, on the new operating system.
The year is 2035. Rajesh Kumar’s father is not a transactional customer. He is a managed asset in a risk pool, covered by a fully capitated health contract with Integrated Healthcare Company for a premium of ₹1000/month. For the past five years, the company has been actively managing its liability by keeping him healthy: biannual checkups, early detection of his pre-diabetes, and lifestyle modifications to control his cholesterol. This is not altruism; it is active risk management.
One night, a tail-risk event occurs anyway: he has a heart attack.
But now, the system’s response is entirely different.
He is taken to the nearest network hospital, a lean, high-throughput facility 10 minutes away.
His data is liquid via his ABHA ID. The ER has his entire medical history before he’s even fully stabilized.
The cardiologist is a salaried employee, not a commission-based agent. His compensation is tied to long-term outcomes, not procedural volume. He makes a risk-adjusted clinical decision to perform a conservative angioplasty.
The system’s own AI flags the procedure for protocol compliance, acting as a real-time, automated auditor against unnecessary up-selling.
The transaction is settled internally. The potential ₹18.4 lakh liability never materializes. The actual cost to the system is ₹2.5 lakh. The amount Rajesh pays is ₹0.
The family’s balance sheet remains intact. The father survives, which is not just the desired human outcome, but the financially optimal one for the system.
This is the future worth building.
It is not a utopian fantasy. It is the logical, inevitable result of a system with properly aligned incentives. The alternative is the machine we have now, a machine that quietly and efficiently liquidates the futures of millions of families every year.
The hospital rake has been a brutally efficient financial instrument for extracting wealth from the Indian middle class for thirty years.
The work of this generation is to invert it. To build a new machine that compounds health and wealth, instead of harvesting it.
For founders building in this space: DM me. For investors deploying capital: DM me. For doctors considering leaving FFS: DM me. For patients tired of the current system: Demand better.
This is the revolution. It’s happening now. Pick a side.
This document is not a conclusion; it is a starting pistol.
What follows is not a “checklist.” It is the due diligence questionnaire for any serious founder, investor, or policymaker considering entering this arena. I have provided the high-level frameworks; this is the granular, unforgiving groundwork.
If you cannot answer these questions with data-backed, high-conviction responses, you are a tourist. You do not have an investment thesis; you have an opinion.
Your job begins now.
Part I: The System
What is the exact legal and contractual mechanism by which a hospital places a lien on a human body?
What is the case law precedent for lawsuits brought against hospitals for this practice?
What is the quantified incidence rate of this practice across the top 20 private hospital chains?
What is the fully-loaded, line-item P&L and cash flow statement for a representative 200-bed, multi-specialty private hospital?
What was the pre-1991 capital structure and payment model for private healthcare?
Which specific clauses in the 1991-1995 liberalization policies created the regulatory vacuum for the FFS boom?
Why did the Indian market structurally reject the managed care/HMO model when it was first introduced globally?
Part II: The Incentives
What is the weighted-average commission percentage paid to surgeons, broken down by procedure category (e.g., ortho vs. cardiac)?
What is the operational flowchart and decision tree for the “estimate desk”?
What is the observable market outcome for a hospital that unilaterally attempts to adopt an ethical, salaried-doctor model within the existing FFS ecosystem?
What is the detailed business model of a Third-Party Administrator (TPA)? How are their contracts structured?
Are TPAs financially incentivized to reduce claim amounts, or do they profit as a percentage of the total claim value?
What is the percentage of total procedure value that is paid by private insurance vs. OOP vs. government schemes?
Why haven’t the country’s largest insurers used their market power to force a shift to value-based care?
Part III: The Insurgent
What is the real estate sourcing and qualification model for SuperHealth’s properties?
What are the standard terms (lease duration, cost/sq. ft., escalation clauses) of their real estate contracts?
How is the risk of lease renewal price-gouging modeled in their long-term financials?
Is the 125-day build-out timeline a marketing number or a replicable, scaled reality? What are the dependencies?
What is the full, exhaustive list of procedures that fit within the 1.2-day ALOS model?
What is the explicit protocol for patients who require longer-term, complex, or ICU care?
How do they contractually and operationally prevent the “patient dumping” of high-cost cases onto other hospitals?
What is the normalized Revenue Per Bed Per Month for a SuperHealth facility vs. a comparable Apollo facility?
What is the unlevered cash-on-cash payback period for a single hospital unit?
At what percentage of bed utilization do they hit unit-level breakeven?
What is the standard org chart and hiring sequence for the first 100 employees of a new facility?
What is the fully-loaded, multi-tranche capital requirement to reach the 100-hospital target?
What are the specific terms of the United Imaging deal? Is it a pure usage fee, a revenue share, or a hybrid?
What is their customer acquisition strategy and CAC for the non-subscription part of their business?
How do they quantitatively prove their “honesty” to the market? What are the KPIs for trust?
Part IV: The Insurgent
What is the detailed, multi-tiered pricing structure for their subscription product?
What is the full list of inclusions, exclusions, and co-pay requirements?
What is their current and target Medical Loss Ratio (MLR)?
What is their quantified strategy to mitigate adverse selection?
What is their underwriting process? What conditions or demographics are excluded?
What were the specific, critical failure points of the asset-light partnership model?
What is structurally and operationally different about Even’s owned hospitals versus a SuperHealth facility?
What is the capital efficiency (EBITDA per dollar of invested capital) of their owned-hospital model vs. SuperHealth’s?
What is the technical architecture for the data flow from their app to their physical facilities?
What is the monetization model, if any, for non-subscribers using Even’s hospitals?
What is the 10-year vision: a healthcare provider with a software business, or a software business with a captive healthcare provider?
Part V: The Convergence
What are the calculated customer switching costs for the SuperHealth model vs. the Even model?
Who has the durable advantage in the race to full-stack: the company that masters atoms first, or the one that masters bits first?
What is the likely endgame ownership structure of this market (e.g., oligopoly, regional monopolies, etc.)?
Part VI: The Enablers
What are the audited unit economics of a Narayana Health cardiac surgery?
What were the specific, binding constraints that prevented Narayana from scaling to 1,000 hospitals?
Can the “heart factory” model be successfully replicated for other, less standardized service lines?
What is the current, verifiable adoption rate of ABHA IDs among the addressable patient population?
What is the technical architecture of the ABDM stack?
Who bears the cost of ABDM integration for providers and patients?
What is the quantified data quality (completeness, accuracy, structure) of the records currently on the ABDM network?
What are the specific privacy and data security risks of a centralized, government-run health data infrastructure?
Which specific incumbent hospital chains are actively resisting ABDM integration, and what are their stated reasons?
What is the precise legal and regulatory framework governing what can and cannot be done via telemedicine?
What is the current liability and malpractice framework for a remote misdiagnosis?
How do the powers of the national telemedicine guidelines interact with the authority of state-level medical councils?
Is there a concrete regulatory roadmap from IRDAI for the adoption of value-based payment models?
What would the specific contractual and financial structure of a “value-based payment” look like in the Indian context?
Which specific insurance companies or state governments are running active capitation pilots today?
Part VII: The Bear Cases
What percentage of total Indian healthcare spending is driven by the top decile of the income bracket?
Is there a statistically significant correlation between hospital price point and patient-reported satisfaction scores?
How will the insurgents overcome the market’s deeply ingrained “price = quality” heuristic?
What is the all-in, fully-loaded compensation for a median doctor at an insurgent vs. an incumbent?
What is the trailing 12-month doctor churn rate for the insurgents?
Where are the specific, scalable talent pools of high-quality doctors who have not been acculturated to the FFS system?
What is SuperHealth’s current case mix index (a measure of patient sickness)?
What happens to their unit economics when a statistically significant number of high-comorbidity patients enter their system?
How can the insurgents quantitatively prove to the market that they are not just cherry-picking healthy patients?
What is the maximum number of facilities a single management team can effectively oversee before diseconomies of scale set in?
Will the real estate arbitrage that underpins the low-CAPEX model evaporate as they scale and become a major market player?
What is the technology and process stack for ensuring clinical quality control across a distributed network?
What is stopping an incumbent from launching a separate, low-cost “fighter brand” to compete directly?
Do the incumbents have a lower cost of capital that gives them a durable advantage in a long-term price war?
How will the insurgents overcome the incumbents’ powerful brand moat?
Part VIII: The Execution
Where, precisely, in the healthcare value chain will you make your initial entry?
What is your specific, unfair advantage against both incumbents and other insurgents?
What is your detailed, 36-month plan to evolve from a point solution to a full-stack player?
What are the five key metrics that investors in this space actually care about?
What is the standard valuation framework for a company at your chosen entry point?
Which specific VC and PE firms have a stated thesis and are actively deploying capital in this space?
What is the total capital requirement, by funding stage, for your specific model?
How, specifically, will you recruit your first ten “true believer” doctors?
What is the ideal founding team composition for your chosen model?
Where are the specific geographic and institutional talent pools you will target?
What is the full, exhaustive list of licenses required to launch your initial operation?
What is the realistic, risk-adjusted timeline for securing all necessary permits?
What are the most likely future regulatory attacks that could kill your business?
Part IX: The Roadmap
What are the five non-vanity KPIs that will prove your model is working?
What is your geographic expansion strategy, and why?
What is your M&A strategy? Do you buy, build, or partner?
What is the specific policy change that would act as a massive forcing function for your business?
What do you believe the market structure of this industry will look like in 2035?
Part X: The International
What is the detailed cost structure of a JCI-accredited hospital in Thailand, Singapore, and Turkey?
What are the specific quality certifications and accreditations that matter in the global medical tourism market?
Can India realistically replicate the Thai medical tourism playbook, and what are the barriers?
What is the detailed financial and operational model of Kaiser Permanente?
Answer these 95 questions with specificity, and you’ll know more about Indian healthcare than 99% of investors, operators, and policymakers. The answers to these 95 questions are not the appendix to an investment thesis. They are the thesis.
Epilogue: Why This Matters Beyond India
Let’s be clear: this was never just an Indian story.
India is the testing ground. It is the brutal, chaotic, perfectly hostile environment in which a new, hyper-efficient model for healthcare is being forged. The real prize is not just fixing India; it is exporting the finished product.
The Series B Markets: The Next 2.5 Billion
There are roughly 2.5 billion people living in countries that are running a slightly different version of the same broken OS:
Pakistan (240M)
Bangladesh (170M)
Indonesia (275M)
The Philippines (115M)
Nigeria (220M)
...and so on.
All of them share the same source code: low public spending, high out-of-pocket expenditure, and a predatory Fee-for-Service private sector.
If an insurgent can make the full-stack, incentive-aligned model work in India, what they have built is not just a company. They have built a Healthcare System-in-a-Box: a repeatable, scalable playbook for delivering low-cost, high-quality care in any structurally similar market.
This is the largest addressable market in the history of healthcare. It is not a bet on serving the 330 million people in the saturated, $4.5 trillion US market. It is a bet on serving the 2.9 billion people in the fastest-growing, most unsolved markets on earth. This is the antithesis of the canonical Silicon Valley playbook, which optimizes for high-margin software sold to the global 1%. This is a bet on volume, operational excellence, and the other 99%.
The Great Reversal: Exporting Scarcity Innovation to the Land of Abundance
But here is the truly beautiful, paradoxical endgame. The company that wins in India will not just expand to other emerging markets. It will, eventually, expand back to the developed world.
Why? Because the developed world’s healthcare systems are slowly, inexorably, becoming more like India’s.
The United States: The American FFS system is just a more expensive, more complex version of the Indian doom loop. ¹¹ Medical bankruptcy is the #1 cause of personal bankruptcy. High-deductible plans are pushing more and more costs out-of-pocket. Trust in the system is collapsing.
The United Kingdom: The public NHS is cracking under the strain of underfunding and overwhelming demand. A private market is rapidly emerging to serve a middle class that is no longer willing to wait.
The system forged in the crucible of Indian scarcity, a system obsessed with capital efficiency, operational throughput, and technological leverage, will look like magic when deployed in these bloated, inefficient markets.
A SuperHealth that can deliver a ₹40,000 surgery in India can enter the US market and deliver the same procedure for $8,000. To the Indian company, this is a 15x price increase. To the American patient, who was quoted $80,000 by a legacy hospital, this is a 90% discount. This is the ultimate arbitrage.
The Once-in-a-Generation Alignment
This is how you build a ₹10 trillion ($100B+) company:
Solve India (1.4B people): Prove the model in the world’s most competitive and complex market.
Scale to Emerging Markets (2.5B people): Export the playbook.
Disrupt Developed Markets (1B people): Export the hyper-efficient cost structure at premium pricing.
No healthcare company in history has ever had this opportunity, because no market has ever had this perfect, fleeting alignment of catalysts:
Public Digital Rails at Scale: ABDM, UPI, and Aadhaar provide the foundational infrastructure.
A Flood of Dry Powder: Unprecedented availability of both domestic and global venture capital.
A Deep, Liquid Talent Pool: Over a million doctors and three million nurses.
A Desperate Government: A political class that is actively seeking, and willing to support, any viable solution.
A Burning Platform: A system so fundamentally broken that the activation energy for radical change is finally present.
All five of these forces are aligned over India, right now. This decade. This window.
The Meta-Lesson: A Generalizable Algorithm for System Change
Strip away the specifics of Indian healthcare, and you are left with a repeatable, seven-step algorithm for executing a hostile takeover of any market that is stuck in a stable but negative-sum equilibrium.
Step 1: Map the Doom Loop.
Every broken system is a self-reinforcing machine. Your first job is not to build; it is to reverse-engineer. You must identify the specific, interlocking gears that keep the machine running. In healthcare, it was a financial doom loop:
High CAPEX → Crushing Debt → Extractive FFS Incentives → High Margins → More Capital for High CAPEX.
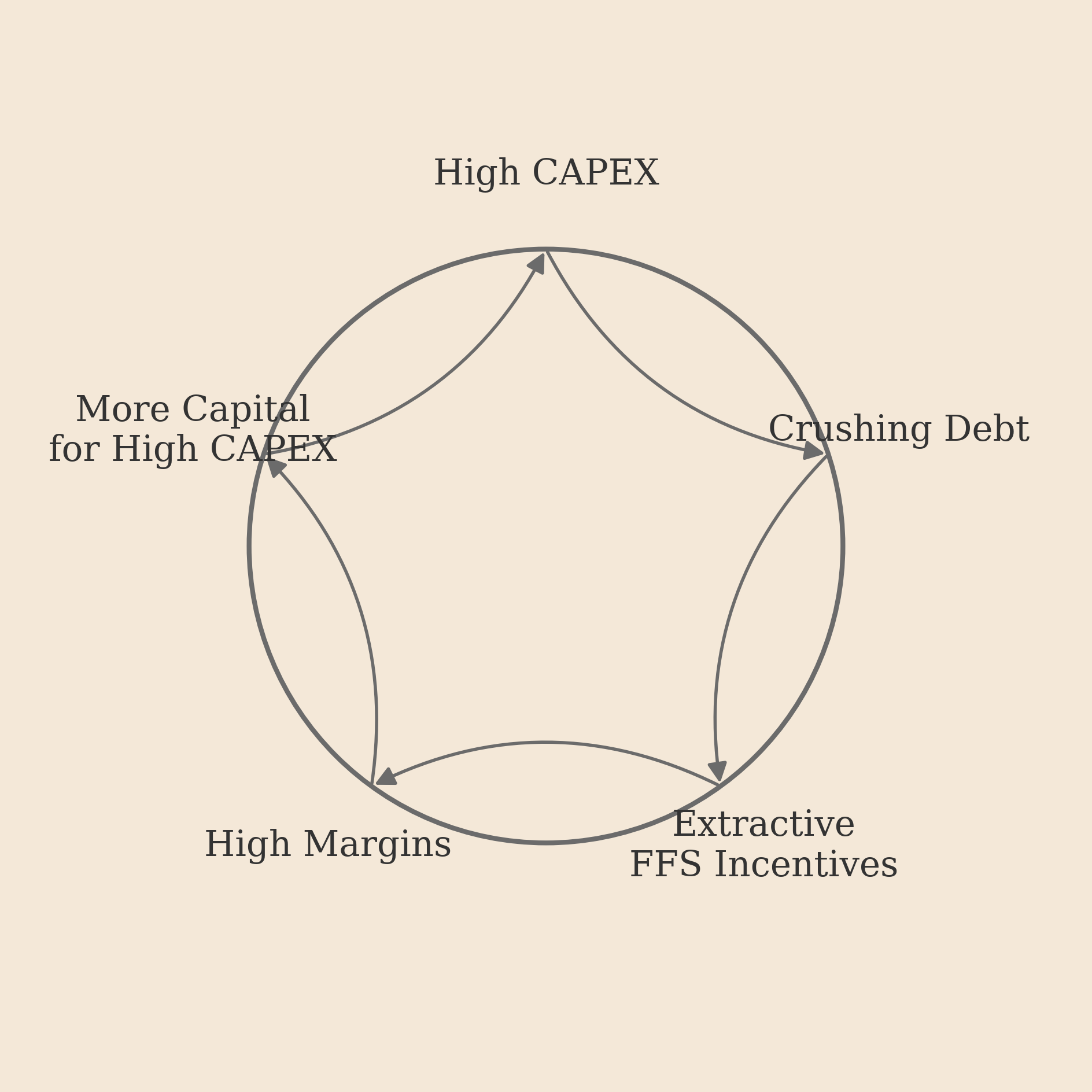
Your target system has its own unique loop. Find it. Map it.
Step 2: Engineer the Inversion.
Once you understand the logic of the old machine, you design a new one by inverting its core incentive. You find the fundamental misalignment, the point where the system profits from its customer’s loss, and you flip it 180 degrees. In healthcare, the inversion was simple: build a model that is structurally long its customers’ health, not short it.
Step 3: Integrate the Hardware and the Software.
This is the crucial, non-obvious step. You cannot run a new, enlightened operating system (the software) on a legacy balance sheet (the hardware). The capital structure and the business logic are inextricably linked. You cannot fix the incentives without fixing the economics, and you cannot fix the economics without fixing the incentives. They must be solved for simultaneously. ¹²
Step 4: Acknowledge the Inevitability of Vertical Integration.
In a low-trust or broken market, the asset-light “platform” model is a fantasy. It is a transitional state, not a destination. Whether you start with the hardware (like SuperHealth) or the software (like Even), the market will inevitably force you to converge on a full-stack, vertically integrated model. You cannot outsource trust. You cannot run your superior logic on a partner’s corrupt infrastructure. Plan to own the whole stack from Day One.
Step 5: Arbitrage the Regulatory Surface.
Do not wait for permission. Regulation is not a static wall; it’s a dynamic, navigable terrain. Find the grey areas. Exploit the lexical arbitrages (”it’s not insurance, it’s a membership”). Use the bugs in the system (like federalism) to your advantage. The goal is to build a product that is so popular and so obviously beneficial that by the time the regulator is forced to pay attention, making it illegal is politically untenable. You adapt to the regulations until you are big enough that the regulations must adapt to you.
Step 6: De-Risk the Unit Economics Before Scaling.
Before you raise a billion dollars to blitzscale, you must prove that your new machine actually works in a controlled environment. A network of ten flawlessly executed, unit-economically positive hospitals is infinitely more valuable than a hundred mediocre ones. The goal of the seed and Series A is not to capture market share; it is to prove, irrefutably, that your new physics is sound. One delighted customer who becomes a missionary is worth more than a hundred who are merely satisfied.
Step 7: Weaponize the Playbook.
Once you have proven that your new model works, secrecy is irrelevant. The revolution becomes inevitable. The market now knows that a better system is possible. Your only remaining moat is execution speed and the trust you build with your brand. Competition from copycats is not a threat but the ultimate validation of your thesis.
This algorithm is modular. You can unplug “healthcare” and plug in any other industry running on a broken set of incentives:
Education: (Incentive: Teachers are paid for attendance, not for student outcomes) → Invert It.
Banking: (Incentive: Maximize fees and net interest margin, not the customer’s net worth) → Invert It.
Insurance: (Incentive: Deny claims to protect the float, not prevent the loss in the first place) → Invert It.
Housing: (Incentive: Maximize rent extraction, not create long-term, stable communities) → Invert It.
Pick your doom loop. Engineer the inversion. Build the integrated machine that makes the inversion profitable.
That’s how you build a generational company.
Final Words: To The Builders
You have now read the full investment memo. You possess the source code for both the broken system and the revolution that will replace it. You are no longer an observer; you are an informed market participant.
The question is, which role will you play?
The System Architect (The Founder): You see the arbitrage. Go build the machine to capture it.
The Capital Allocator (The Investor): You see the thesis. Your job is to underwrite the right architects.
The Key Human Asset (The Doctor): You are the most critical, constrained input in this entire equation. Your choices will determine the velocity of the revolution.
The Market (The Patient): You are the ultimate source of the demand signal that will either starve the old machine or fuel the new one.
The Rule Setter (The Policymaker): You are the designer of the game board on which this will all play out.
You now understand the core physics of this market:
The Inefficiency: The CAPEX-Incentive Doom Loop.
The Arbitrage: The full-stack, incentive-aligned model.
The Catalysts: The convergence of new technology and regulation.
The Risks: The five horsemen of talent, trust, scale, incumbents, and capture.
The Endgame: The potential to build a global, trillion-dollar company by exporting a better system.
Most importantly, you know that this is not a fantasy. It is possible.
The next decade, therefore, is a fork in the road. It is a choice between two distinct futures.
The outcome is not preordained. It will be determined by the actions of the builders.
To the Founders: Your job is to protect the integrity of the new algorithm. The system will constantly tempt you to re-introduce the profitable bugs of the old one, a hidden commission, an unnecessary test. The moment you compromise, your alpha decays to zero. You become just a more efficient version of the old machine.
To the Investors: The asset-light, top-of-funnel plays are a crowded, low-moat trade. The full-stack, vertically integrated models are the capital-intensive, high-conviction, generational trades. Underwrite the architects who are building the entire cathedral, not just decorating the lobby.
To the Doctors: The FFS system is a cartel that only functions because its most critical suppliers, you, agree to its terms. It has monetized your skill, but it has also corrupted your craft. If 20% of you walk away, the cartel breaks. Be the 20%.
To the Patients: You are the market. Every rupee you spend is a vote. Your choices create the feedback loop. Starve the opaque, extractive systems. Feed the transparent, value-aligned ones. Your demand is the selective pressure that will determine which model survives.
To the Policymakers: Your job is not to pick winners. It is to be a ruthless market designer. Regulate the outputs, not the inputs. Mandate radical transparency on clinical outcomes and all-in pricing. Make the data liquid. Then, stand back and let the best algorithm win.
This is the story of Indian healthcare in the 2020s. A system so perfectly broken it worked flawlessly for the few. A handful of insurgents who saw the arbitrage in building a better one. And the decade-long window to see if they can pull it off.
One Last Thing.
Look. This document is a snapshot, a single frame in a long movie. It has a shelf life. The specific numbers in this memo will be wrong in six months. Some of the companies mentioned will pivot, merge, or die.
But the underlying physics of the trade are timeless.
The core thesis does not decay: Markets built on a foundation of deeply misaligned incentives are not in a stable equilibrium. They are, by their very nature, a pot of alpha waiting to be harvested by a better model. ¹³
Indian healthcare, as currently constituted, is one of the largest, most structurally misaligned markets on the planet.
Full-stack, integrated care is the arbitrage.
This market correction is, therefore, inevitable.
The only open variables are the timeline and the names on the cap table.
“The best time to fix Indian healthcare was 30 years ago.
The second-best time is now.”
¹One might argue this is legally dubious, and one would be right. There is no explicit law permitting a hospital to hold a body for non-payment. However, in the absence of a law forbidding it, hospitals often assert a “right of lien,” similar to a mechanic keeping your car until you pay for repairs. The human body is treated, for the purposes of the transaction, as chattel. Most families, facing a combination of grief, social pressure for funeral rites, and a lack of resources for a legal fight, simply pay.
²One could argue the true principal here is not even the hospital’s management, but its balance sheet. The doctor and the hospital administrators are both merely agents executing the cold, mathematical logic of the capital structure they’ve created.
³This is the classic “scaling the founder” problem. A system built on the singular vision and operational intensity of a figure like Dr. Shetty is incredibly hard to replicate once you need layers of middle management. The culture that works at one facility gets diluted by the 10th and can be unrecognizable by the 30th.
⁴Asking an incumbent hospital chain to embrace ABDM is like asking a 1990s investment bank to publish its proprietary trading algorithms for free. The information asymmetry is the source of the alpha.
⁵TPAs are a fascinating animal. They are theoretically neutral administrators, but their contracts are often structured in a way that rewards them for reducing the claim amount, either through negotiation or outright denial. This makes them less of a referee and more of a second, even more cynical, line of defense for the insurer’s balance sheet.
⁶Corporate culture is, in many ways, a temporary substitute for perfect contracts and infinite oversight. A strong founder-led culture aligns employees around a shared goal in the absence of explicit, enforceable rules for every possible situation. As an organization scales, it becomes impossible to maintain that cultural cohesion, and it must be replaced by the very thing it sought to avoid: process, bureaucracy, and formal contracts.
⁷This is the core of the dilemma. The rational, NPV-positive decision for the incumbent in the short term is always to double down on the existing, high-margin business. By the time the new, disruptive model has grown large enough to be a material threat, the incumbent has lost the institutional muscle and market position to compete effectively. See: Blockbuster vs. Netflix.
⁸This is a classic example of pricing in systemic friction. The consultant’s fee is not for their influence, but for their knowledge of the process and their ability to ensure your file doesn’t get “lost” at the bottom of a stack. It is a cost of doing business in an inefficient system.
⁹Being a non-profit is great for mission alignment and tax advantages, but it makes you structurally dependent on retained earnings and debt for growth. You can’t just call up a VC and raise a billion-dollar growth round to blitzscale into a new market. This is a fundamental governor on your potential speed.
¹⁰This is the ultimate moral hazard of the system. The FFS doom loop is a Nash equilibrium. It’s the state to which the system will naturally revert if not held in check by an external force. In this case, that force has to be the founder’s own integrity, codified into the company’s DNA.
¹¹The fundamental difference is that the American system is a B2B sale to large insurance companies and employers, whereas the Indian system is a brutal, direct-to-consumer, cash-on-delivery business. This has forced the Indian incumbents to perfect the art of extraction at the individual level, a set of skills that, ironically, makes the Indian market a more demanding and competitive training ground.
¹²This is the central fallacy of a thousand failed “disruptions.” A brilliant app that tries to bring price transparency to a market (like healthcare) will fail if it doesn’t also solve for the underlying capital structure that requires price opacity to survive. You cannot just build a better UI for a broken system.
¹³This is the closest thing to a first law of thermodynamics for markets. A system that consistently generates negative externalities for its customers in order to create profits for its owners will eventually face either a catastrophic collapse or a hostile, top-to-bottom disruption. The energy required to maintain the misalignment eventually becomes too great. The only question is the timing of the catalyst.
How the hell you have done research Man
Its a Masterpiece
Fabulous article! This is pretty deep analysis and loved it. Also super bullish on both even and superhealth